
Episode 7.5 Breech Delivery Tips, Laparoscopy Entry, and IVF Legality
In this episode, we discuss four tips for breech vaginal delivery. Then, we respond to the Alabama Supreme Court’s decisions about embryos and the impact on IVF and reproductive rights. Finally, we discuss the best methods for initial laparoscopic entry and discuss the history of laparoscopy.
00:00:02 Four Tips for Vaginal Breech Deliveries
00:13:17 Alabama Supreme Court and IVF
00:29:15 Initial Laparoscopic Entry
Links Discussed
The Evolution of Laparoscopy and the Revolution in Surgery in the Decade of the 1990s
Vascular injury at laparoscopy: a guide to management
Laparoscopic entry: a review of techniques, technologies, and complications
Transcript
Howard 00:17
Antonia.
Antonia 00:18
Howard.
Howard 00:19
What are we thinking about on today’s episode?
Antonia 00:21
Well, we’re going to talk about the recent legal challenge essentially to IVF and also about initial laparoscopic entry, but first we have four tips for breach vaginal delivery. Now we’re assuming that the listener already has some basic training at least in doing breach deliveries and knows the delivery maneuvers. We just want to build on that a little bit with our core tips. So I’ll say a big initial step is appropriate consent and selecting the right candidate, though a lot of these also happen in maybe less optimal emergency situations where the woman might present an advanced labor with a breach fetus. So those things are maybe a bit beyond what we want to discuss today. In those situations you just do what you can. But this is more for controlled situations where there’s a breach vaginal delivery.
Howard 01:18
Well, I think most breach deliveries are unintentional at this point, apart from, say, second twins. There’s a lot of overlap between delivery of a second twin that’s breach presenting and a singleton breach delivery. But technically these are two different procedures. We call the first scenario with an aftercoming twin a breach extraction and to distinguish that from a breach delivery, and the difference primarily involves how quickly you move to doing active things during the delivery. With a singleton you have to be really patient and not rush things. Specifically you have to resist extracting them, pulling too soon. But with a breach extraction of a second twin you can go pretty much as fast as you want to go.
Antonia 01:56
Okay. So then the first tip here is avoid this situation entirely, if you can. So with appropriate counseling and doing an external cephalic version versus even a planned cesarean if the UCV doesn’t work, or they decline it or it’s not appropriate. So we already talked about UCV in a different episode pretty recently. But why don’t you tell us why this is a tip for breach deliveries?
Howard 02:24
Well, I think it’s one of those things, just like how you avoid complications of a cesarean, for example. The tip there is do fewer cesareans, don’t do the unnecessary cesarean to begin with, and you avoid complications. So how do you avoid complications during hysterectomy? Don’t do hysterectomies unless you need to them, and then do it in the most minimally invasive way and try to avoid doing the thing to begin with. So the same thing’s true here as we discussed before. External cephalic version is effective at reducing the number of remaining breach pregnancies out there in the world, and that means fewer cesareans for breach, but it also means having to do fewer potentially risky breach vaginal deliveries. Even by conservative estimates, we should be able to cut these numbers at least in half if we routinely offered and performed external cephalic version to our patients. But I would encourage folks to listen to our discussion of that a couple of episodes ago. There’s no doubt that we’re not doing enough external cephalic versions, in the United States at least.
Antonia 03:21
Okay. So the first tip is don’t even do it if you don’t have to or don’t wind up in that situation. Second tip here would be simulation. So breach deliveries are rare enough that simulation is going to be the only feasible way for any provider, in the modern day US at least, to get the necessary reps to stay current because, like we just said, most breach babies are eitherverted or sectioned. So a lot of OBGYNs will be lucky, frankly, to do a breach vaginal delivery even once a year. If that most people would do it far less often. But it’s a very unique skill set. So it’s something that if you’re going to do it, you’re not going to get a lot of other ways to practice it. The only other opportunities we get to use even some of those skills would be breach second twins or breach cesareans, but it’s not exactly the same thing.
Howard 04:19
Yeah, and even then a typical OBGYN might only do three or four of those per year, given how rare those things are. So simulation plays a huge role in going through the steps and rehearsing unusual and emergency scenarios that might arise. This doesn’t have to be anything fancy a simple low-fidelity pelvis with a low-fidelity fetal mannequin. It’s all you really need to go through various scenarios and practice the technical steps involved in doing a breach delivery. Now it is helpful to think about scenarios ahead of time that might arise, that are challenging or which present to your learners or yourself or your colleagues something other than the normal and what you might not be looking for.
Antonia 05:01
So you can think of scenarios you’ve come in contact with in real life on unintended early preterm, precipitous breach delivery might be one thing, another one might be a nucle arm or incomplete cervical dilation, or cephalopelvic disproportion, maybe cord prolapse with a, a breach presentation, or fetal bradycardia, or even just fetuses that are facing up, so sacrum posterior.
Howard 05:31
Yeah right, all of those would be excellent simulations to drill for, and I might include a short umbilical cord and an entrapped head. Obviously, you mentioned undilated cervix, but also a bony entrapment of the head, so each of those have specific management procedures and listeners are interested. We can talk about those in detail at another time perhaps, but a simulation exercise would also just include a review of contraindications and prerequisites to breach fetal delivery and then, of course, all the normal steps that we haven’t really mentioned and the procedures that you would do during a delivery. So things like the pinard maneuver or the luffset maneuver, merisosmeli bite maneuver, things like that.
Antonia 06:10
I’m getting flashbacks. Now to the eponyms episode.
Howard 06:14
Flashbacks? Do you mean fond remembrances?
Antonia 06:16
I don’t know about fond, how many of those maneuvers were named after women again.
Howard 06:22
Okay, all right, well, we can move on. I think.
Antonia 06:24
That’s what I thought. Okay. So second tip with simulation. Third tip is being hands off as much as possible and being patient all the way until the end. So all the way, basically, until you’ve just got the head to deliver, and maybe even hands off till then as well. And I think personally there was a pretty nice depiction of this early on in the Call of the Midwife series on Netflix.
Howard 06:49
Early on. I think that show is still going on now and it’s 12 years old. But yeah, patients comes in two forms here Patients with a C. The first thing is that you want to let the breach patient labor down and not encourage pushing too soon. So early pushing at complete dilation doesn’t apply here.
07:08
We’ve talked about how it’s recommended for cephalic pregnancies to go ahead and push when you’re dilated, but for breach deliveries it’s the exact opposite. It’s incredibly important to wait. So after she’s completely dilated, just keep waiting as long as the fetal tracing is good. You want to see the breach spontaneously distending the mother’s perineum before you ever start to push. This gives more time for the cervix to dilate. It also helps to prevent extension of the arms and legs. Then, with pushing, which could be up to an hour later for nalliparous patients and at least 30 minutes for a multiparous patient, you want to be patient here as well. Resist the urge to grab or pull on the baby Now at this point. As you said, it’s completely hands off If the breach is riding up the perineum, which is another way of saying crowning, but the word crowning only applies to the crown of the head, so we don’t use it here.
07:57
In this case we say riding up, and it’s sacrum posterior, one of those scenarios you mentioned Then you’ll want to rotate that to sacrum anterior and as the thighs become visible once you can see the knees at least then you can assist the delivery of the legs, not by pulling outward, just by flexing up and sweeping.
08:14
You can also assist during this time by keeping the head flexed with your abdominal hand or with an ultrasound transducer if you need to, and this will help ensure that the head engages the pelvis in the correct way, meaning flexed, and once the legs and umbilicus are out, you can pull down a piece of cord and feel the heartbeat and also make sure it’s not too short. That’s part of that short cord scenario I mentioned. And if you see the elbows or shoulder blades, you can assist to deliver the arms by flexing and sweeping. Again, I’m not going to use an epineum, but here’s the last bit of patience. So you’ve delivered the arms and legs and you’re so anxious to get that head out and the temptation is to pull on the breach. But you really are waiting for the nipples, even the shoulders, to be delivered spontaneously with the engaged head, until you do any pulling or any other kind of assistance to deliver the fetal head.
Antonia 09:04
Yeah. So this is a big rule, because you see a baby’s body hanging out like that and you really want to do something. But you are already doing something. You’re making sure the heart rate’s okay, the sacrum is anterior, the head is flexed and engaged and then at the very end, basically when you can already reach your fingers up to their cheekbones, that’s when you’re ready to do that epineum, more so smelly-white maneuver. So it really takes them conscious application of patience to avoid rushing things and specifically avoid pulling on that baby’s body to get that head out, because then you’re more likely to just pull the head down into a cervix that’s contracting around it, or pull it down into an extended position where it could even be like a bony entrapment, which both of those would really be not good. So be patient. And our last tip here is have Piper’s forceps available and know how to use them.
Howard 10:07
Yeah, I think the point is not that you need to use Piper’s that often, but that you need to think about them and have them ready anytime you’re potentially doing a breach delivery, including at the time of Caesarean.
10:18
The place where most of us are going to occasionally need them and get practice is during a difficult breach extraction at the time of a Caesarean delivery, and when you need them, you need them now.
10:28
So that means you need them in the room or even on the field, which means you need to have some forethought about it and you need to have told your staff that you need them and have them ready before you end up needing them in an emergency. But also, putting them on and using them in simulations or, as needed, during breach Caesarean is a great opportunity to practice using them for those rare breach vaginal deliveries where you need them and you need to know how to use them well to make a big difference. They can be quite useful during Caesarean’s, where the head is difficult to extract. So don’t be afraid of them and make sure you have them in the room and use them when you’re struggling and learn how to use them in simulations so that when the time comes with that surprise 3am breach, delivery in a cervix, that a patient that didn’t have a chance to labor down and all that. You can use them to get that head flexed and accomplish the delivery.
Antonia 11:17
Yeah, I will say that you need room for Piper Force Epsom. The only time I’ve ever actually asked for them was during a Caesarean, and in that case I had to extend the uterine incision just to fit them on. But then when I did, then the baby just came out fine without needing the assistance of the Force Epsom. But obviously you can’t always do that, especially in a vaginal delivery. You can’t just extend the vagina, so to speak. You can, but that is a lot harder to repair.
11:48
Anyway, most breach deliveries today, which are still few and far between probably well, I don’t know about most, but probably a good amount of them are done outside of the labor ward, whether that’s in an ambulance or in the ER, because it was unplanned and precipitous or possibly in a planned breach home birth scenario. So either way, it’s probably involving people who are not listening to this podcast. But if you work in an emergency department, it’s probably a good idea to do some kind of course like ALSO, or ECO is another one, so that those are advanced life support for obstetrics, and I believe that’s by the AAFP. And then emergencies in clinical obstetrics is another one, because you never know when someone’s going to pop into your ER with some part of a baby hanging out between their legs. So you just want to know how to act fast.
Howard 12:43
A butt, a cord or something.
Antonia 12:45
yeah, yeah, Okay. Well, let’s shift gears now and talk again about IVF First. So we talked we answered a listener question last time about freezing eggs, so I wanted to make a little correction to something I said. I was talking about how donor embryos are not really adopted, because once they’re in your body and you give birth to them, it’s by default you’re a child. It’s not adopted. Obviously, that’s not taking into account surrogacy, but I don’t think that that was exactly relevant to our listener’s question. Surrogacy still requires a legal agreement to get around that default parent issue.
Howard 13:24
And those issues vary by state. So anytime you’re doing these sorts of issues, you really should see your state’s laws and have a lawyer. Drop all the paperwork with the intended loopholes. Jump through before you go through with it.
Antonia 13:37
Yeah, yeah.
Howard 13:38
Well, it’s a complicated world, so there are cases, though, where they might lose custody for some reason or things come up and, like I said, it varies step by step by state law, so if we told you the laws in our state, it may not apply to yours.
Antonia 13:51
Yeah, there really could be exceptions to anything I say, so just fact check me. But I also and you also, I think wanted to talk about IVF because of the legal developments and these are very recent since our last episode. So I’m talking about the Alabama Supreme Court ruling on the legal personhood of frozen embryos. This came as a little bit of a shock to me. Maybe it shouldn’t have, but somehow I always trusted that IVF was protected, even in the setting of increased abortion restrictions, because in my mind I thought IVF is a very pro-life thing to do. So surely that will still continue. And then, when this ruling came out, I thought well, surely the lawmakers didn’t intend for this, for IVF to get banned because of this personhood ruling, and surely they’ll swiftly correct this. It’s been not gonna disrupt all the lives of all of these fertility patients in Alabama, and it’s by the time our next episode comes out. It’s gonna be a moot point, but that is so far not exactly happening. Maybe it will soon, but now I’m not so optimistic anymore.
15:08
So this case that happened.
15:09
My understanding is there were some frozen embryos for some IVF patients that were not properly secured and some random person walked in and got ahold of them out of the freezer and just destroyed them, which I have some questions about that and how that happened.
15:26
But anyway the families sued and over the process of that lawsuit it was declared that those embryos that were destroyed were people and that meant they were subject to the same wrongful death and murder statutes. That also applied to children and in Alabama applied to unborn fetuses, like unborn children that are in utero. So now they just applied this also to frozen embryos. So this is not the first time that frozen IVF embryos have been unintentionally lost by some kind of mishap. Most, if not all, ivf clinics do already have waivers that the parents sign indicating that they understand the risk of accidental loss for technical issues the power goes out or other storage conditions, for example and that they release the clinics of liability, and sometimes even despite these waivers, there have been cases in the past where families have been successfully able to sue for damages, but those cases it’s been either emotional damages or for loss of unique property, not murder. But now in Alabama they’re bringing in personhood and they’re equating it at least with manslaughter.
Howard 16:41
Yeah, and in this lawsuit the patients did sue for wrongful death of their embryos and a lower court initially, as I understand it, rejected this claim. But the Alabama Supreme Court upheld their claim and they were very blatant about citing at least one. Justice was about citing their Christian religious beliefs in the ruling, which is interesting in itself. But already, as a result of this, I think most of the in vitro programs in Alabama have paused their services and from what I understand in my role as a legislative chair for District 7 of ACOG, which includes the state of Alabama, there’s no obvious or immediate pathway to resolving this issue. It would take the Alabama legislature passing a law specifically saying that embryos are not persons and that in vitro fertilization and other assisted reproductive technologies can proceed without fear of prosecution.
17:31
There has been a law that would decriminalize physicians and, I think, other healthcare workers working its way through the Alabama House. That’s different. Decriminalizing them from prosecution. Basically granting immunity under certain circumstances is a different thing from not counting the embryos essentially as persons, which, as I understand it, they’ve not done. We’ll see how that goes, but also appreciate that that’s not quite enough because it still complicates how we handle the embryos. In other words, we’re saying it’s illegal and it is that, but we’re going to, for political and expedient reasons, not prosecute you for it or decriminalize it. It’s not quite what we need in dealing with embryos, with advanced reproductive technologies and other ancillary medical issues.
Antonia 18:18
Yeah, it seems like nobody really wants to challenge the personhood anymore. They’re afraid of that, so they’re going, they’re taking other avenues. But the immediate fallout, which included halting all embryo transfers and anything that would create new embryos I mean, they’re not even shipping embryos out of the state because they’re worried that that will damage them that is obviously very upsetting and disruptive and it seems like it was probably not the goal, and so that’s. That seeming lack of foresight is honestly quite enraging to me, and of course, it also hits home because I used IVF to get a very chunky and beautiful little boy, but 2% of all children in the US also do that, so this applies to one in 50 living people in the US.
Howard 19:14
Yeah, I think a lot of the issues that we’ve had since the Dobbs decision in various states are even being generous here are due to not understanding the implications. So obviously, by this logic, an ectopic pregnancy or dealing with an ectopic pregnancy with methotrexate would be even worse. I mean, that’s actually implanted in some part of your body, and birth control issues and things like that, and so this is what happens when you have legislators that don’t understand the basic science of human reproduction, passing laws in a binary way, and I don’t think the justices here were thinking this through either. As I said, at least one of them justified the argument and the decision by quoting God. He was also already known for being staunchly against abortion, apparently also based upon his interpretation of the Bible, and so that’s normally not how we interpret constitutions of states.
Antonia 20:05
Right, and it strikes me as ironic to see how what I think of as extreme and inflexible views on pro-life and personhood actually turn into anti-life consequences. So we’ve already seen this, where anti-abortion laws will end up limiting also access to birth control and then that paradoxically increases the rates of unintended pregnancies and abortions, even illicit abortions.
Howard 20:35
Yeah, I will say that IUDs have done more to decrease the number of abortions in the United States and pro-life movements ever done.
Antonia 20:42
Yeah, and now with this frozen embryo ruling, it’s going even more backwards and more anti-life, because the risk of some kind of human or technological error that might happen during the handling of frozen embryos just is not gonna be worth these REIs and their clinics and the shipping companies being charged with murder and losing their careers and their livelihoods over. So they’re just not gonna do it now without some kind of legal protection, which necessarily means that we’re preventing thousands and thousands of people who entered this IVF process yearning to become parents, we’re preventing them from having children and then we’re also preventing their existing frozen embryos from living. So that just is not pro-life to me. There’s lots of public rage about this, of course, and we’ve already been seeing news stories about a political scramble to clean this up and proposals for different laws protecting IVF from these at least wrongful death penalties, but then we also see obstruction from other politicians who somehow inexplicably want these IVF restrictions to continue.
Howard 21:57
Well, they may say that they still support in future fertilization, but they also want every single embryo to be saved. I guess they don’t understand that in the process of creating life with in vitro, non-viable embryos are also created, because that’s just how nature works. And they also don’t accept that sometimes there are extra embryos that families can’t keep, but the vast majority of the embryos created are not compatible with life.
Antonia 22:23
Yeah, and on that latter point, I guess they wouldn’t wanna be the ones paying indefinitely for storage of that surplus embryos that the families can’t keep. But then they’re not allowed to be discarded either. But Someone should tell them that a fertilized egg often will either lead to a miscarriage or sometimes more rarely, an invasive cancer and not a person. So you really can’t know. Is this fertilized egg even potentially like, remotely potentially going to be a human, as opposed to a molar pregnancy or miscarriage until it’s developed way beyond the five-day blastocyst stage? And for that to happen it has to implant in the body. We can’t just we don’t grow fetuses yet in test tubes. Maybe one day in the future.
23:15
And this is just such a unique scenario that there’s not really a lot of good analogies to help people understand. But I think the closest thing I can think of is it’s somewhat analogous to assigning personhood to a dermoid cyst, because that has parts of what you might also find in a person. It has teeth and hair and skin, but it is never, ever going to become a person. It’s not a person, it never will be, but it has parts of a person, and so that’s how I view it. So this Alabama Supreme Court ruling already is just biologically wrong.
Howard 23:52
Well, and it’s even worse than that, though. The logical extension of this ruling is that every fertilized embryo from natural intercourse is a person, even before those embryos are implanted. So and don’t get me on slippery slopeism, because we’re living in the slippery slope, so I’m allowed to make these point this can easily lead to restricted access to birth control, because many people will argue, incorrectly, that birth control prevents implantation, and there are people doing that in various states. But think about this 15% or so of all fertilized embryos in natural intercourse fail to implant. The rate of failures even higher with IVF transfers.
24:29
And what do we do about the wrongful deaths of all those naturally conceived embryos? Every sexually active woman in the luteal phase of her menstrual cycle is potentially pregnant with an embryo in the fallopian tube or not yet implanted into the uterus. So if I do something that potentially hurts the mother that could be a medicine, that could be a trauma, it could be a car accident, I don’t know Well then someone could argue that I disrupted the implantation of a pregnancy that was going to implant, and then I’m guilty of murder or manslaughter under this new ruling.
Antonia 24:58
Yeah, and it would just be presumed because it wouldn’t even show up on a positive pregnancy test, so it would be just the suspicion of it and it really sounds ridiculous. But it’s not farfetched at all for people to get blamed and actually criminally charged for spontaneous losses. There was some. A lot of our listeners may already have heard of this. There was a case in Oklahoma in 2021 where a woman was charged with manslaughter and jailed for having a 15-week miscarriage. The logic was that she used meth, so it must have been her fault. But that’s completely lacking medical knowledge, because meth actually is not any more likely than tobacco to cause a miscarriage. I mean, it’s a bad thing to do, but yeah.
Howard 25:43
That’d be actually less. Why don’t we arrest all of the folks who’ve ever smoked tobacco, smoked while they were pregnant and also had a miscarriage?
Antonia 25:49
Yeah, or second hand or third hand smoke. I mean slippery slope right. And just going back to the whole religious tie-ins, I think it’s especially ironic because in the Old Testament of the Bible the fetus is specifically given less worth than the mother, and I’ll explain that here in a second. And there’s also distinctions made between intent, when there’s someone is harmed or is killed. So there’s different consequences if the harm or the death happened accidentally versus from intentionally harming them. And then there’s even an in-between where it was an accident but it was an irresponsible accident.
26:31
So in the book of Exodus there’s all these rules laid out for their society at the time, and one of them says that it gives an example of an irresponsible injury or manslaughter of a pregnant woman, and they say it’s punishable by eye for eye, life for life. So whatever the injury was, that’s the punishment for who did it. But then if that same action only results in miscarriage and not her dying but just her fetus dying, then it’s a different penalty. It’s just that the father of the fetus can demand what he wants. So it’s not death penalty for the perpetrator, as it would have been if the pregnant woman herself had died, and if it’s completely accidental, then the perpetrator. They have to flee, but they will be spared of any other punishment. They won’t get the death penalty.
Howard 27:22
Well, perhaps you can debate the theologic merits of it with the Alabama Supreme Court justice. But yeah, but these rulings don’t have explicit support. Last time I read the New Testament, it doesn’t mention in-between fertilization or any of these things, and certainly not the US Constitution.
Antonia 27:38
But in any event, yeah, so I hope we get some mail about this.
Howard 27:43
Yeah Well, we may have an update on the next episode. One could easily write a dystopian novel about the potential consequences of the slippery slope reproductive power plays. Victims of rape and incest are already being forced to carry pregnancies, as are women who are carrying fetuses with fetal anomalies, like anencephaly, that are completely incompatible with life, but they’re forced to carry them at their own physical expense and potential death. They’re not getting access to the safest medications to treat miscarriages and missed abortion and that’s, of course, not even close to a concept of abortion. And women with previable membrane rupture or women who are bleeding heavily in early pregnancy? We’re wanting them to become septic or go into hemorrhagic shock before doctors feel like they’re allowed to treat them. And now we’ve created a standard where people who desperately want children can’t have them because the natural losses that occur in the process of having a baby through in vitro fertilization aren’t acceptable to an Alabama Supreme Court justice. So it’s a dangerous slippery slope indeed.
Antonia 28:49
There’s just way too much here to keep ranting on, so I think we should stop for now. I feel like my blood pressure is probably going to get high.
Howard 28:57
Well, here’s everyone’s friendly reminder to channel your anger and indignation into something productive lobby advocate, vote for your interest, vote for your patient’s best interest honestly, but let’s not cause your blood pressure to be high, and we can talk about something else for a few minutes.
Antonia 29:10
Yeah, I don’t want to stroke out. Well, this isn’t over. We’re watching the lawmakers very closely, but let’s do move on for now and discuss something else entirely. So we’ve been wanting to discuss laparoscopic entry for a while. It’s just been on our back burner because it’s something we do all the time and there’s a few different approaches. About 50% of complications from laparoscopic surgery occur from the initial entry into the abdomen. So there’s some things to consider here. The first consideration is where does that first trocar go? There’s different variations commonly practiced, including the umbilicus below it or above it at Palmer’s point, or even some modification of that, and probably even some less commonly utilized ones like right upper quadrant or super pubic, all in the context of GYN surgery. And then there’s a question of how to place it. So we’ve got optical direct entry with the trocar, blind direct entry with the trocar, blind entry with a varus needle, and then the open or Hassan technique, and All of these have lots of other little variant details like what position is the patient in and what brands Trocars, what sizes, etc.
Howard 30:26
Yeah, it’s a very complicated topic, like all things in surgical procedures are, with lots of different permutations and combinations and lots of just Handed down conventional wisdom about the pros and cons of each technique and how to do them, and All this stuff develops over time through trial and error and sometimes becomes ingrained in our minds. But I do think we can boil it down into a few principles of best practice, and we can also talk about what to do when things go wrong, if we have time.
Antonia 30:54
The main sorts of injuries that we’re trying to avoid, of course, are injuries to viscous hollow like the bowel or bladder, and, perhaps more importantly though, entries to major blood vessels like the aorta or vena cava or major branches of those vessels as you’ve said, a lot of this has developed by trial and error over the years and then by reactions to various complications, often tend towards being reactionary to complications, and Sometimes these are beneficial reactions, and sometimes we actually swing so hard in the opposite direction that we end up just making things worse. But if we have an injury to a patient, then we’re very likely to change what we’re doing in some way to avoid ever having that same injury again, without often realizing that there’s trade-offs to that change in our technique. So everything has some pros and cons and nothing is entirely risk-free.
Howard 31:48
Yeah, well, that’s right, and I think that the understanding, at least briefly, the history of laparoscopy and how we put that initial short car in will help us Understand some of those reactions that happened over time that have given us so many permutations today.
Antonia 32:01
Yeah, we need our historical tidbit, so why don’t you go into that? That is this episode too yeah.
Howard 32:06
I’m gonna stick to schedule. Well, believe it or not, in 1805 Philip Bosini created a cystoscope that used candles and mirrors to be able to look inside the ladders of dogs. Originally he never used it on humans, but the idea of essentially using a small periscope to see inside of a cavity was born. The equipment got progressively better over time and eventually electric lights were used, and throughout the 19th century different folks Perform cystoscopy or proctoscopy in humans. This was also used for vaginoscopy and eventually Hysteroscopy. And then finally, in 1901 a surgeon named George Kelling inserted a cystoscope through the abdominal wall of a dog to study the effects of Insufflation. He was interested in establishing a pneumo peritoneum to tamponade bleeding as a treatment, but he had the idea to use the scope to see what the effects would be and observe him directly. And then he eventually did this to humans, against a lot of criticism at the time from his colleagues, but he published his findings in 1910.
33:04
The term laparoscopy itself was coined by Swedish surgeon Hans Christian Jacobius, who by 1910 had done 17 laparoscopies with pneumoperitoneum and two thoracoscopies. Interestingly, general surgeons lost interest in this idea very early on and those early pioneers were very criticized by their colleagues. But gynecologists continued developing this technology and the ideas behind it. In 1933 a gynecologist named Carl Fervors used coterie to perform lysis of adhesions laparoscopically. So this was really the first operative laparoscopy, if you will, rather than just diagnostic, and Folks have been using it as a diagnostic tool to look for adhesions or endometriosis or other things before that time. Three years later, in 1936, a Swiss gynecologist named Barsh used cautery to perform a sterilization for the first time and suddenly that became a very important surgery that we could do with laparoscopy.
34:00
In 1932, varus invented his spring-loaded needle, originally to perform therapeutic thoracentesis, and he published a paper on this in 1938. In 1939, to lend very famous gynecologist, pioneered a colposcopic approach to pelviscopy with patients in the lithotomy position, and this actually became very popular for a while. In 1944, decker promoted putting patients in all force positions in a special chair and then putting the scope in the posterior cul-de-sac To look around. Also that year Raul Palmer, very famous gynecologist, used a spring-loaded needle, meaning the Varus needle, and put patients in trend Ellenberg position with insufflation from gas. That was continuously monitored and that was a big breakthrough. That kind of modernized what we do today. Eventually, another gynecologist, Kurt Sim, invented the automatic insufflator in 1960 and started a company that you’ve probably used the products from.
Antonia 34:59
So all of these people were gynecologists, except for Varus.
Howard 35:03
Well, yeah, of course were the pioneers. Now, after 1960, that means all the tools essentially were in place to do what we would call modern laparoscopy, where we put a Varus needle, usually in the umbilicus and Insufflate the abdomen and then put the patient in trend Ellenberg’s position and use what limited tools are available, like cautery, to do more and more things, but mostly tubal ligations. Then doctors like Patrick Steptoe and others were doing more diverse procedures that popularized this approach. Steptoe, of course, was very instrumental in in vitro fertilization creation. Remember, back then you had to harvest the eggs with laparoscopy because you didn’t have ultrasound and got a needle.
35:41
By the 1970s Everyone wanted to go take a weekend course and learn how to do laparoscopy, mainly to do tubals, and then buy equipment at their local hospital which was being heavily marketed by Kurt Sims company and others at that point. And by 1976 60% of all tubal ligations in the United States are being performed laparoscopically. This was at a time when general surgery was really doing nothing at all with laparoscopy. So there was this period of quick adoption and almost irrational exuberance by Gynecologists over a few year time period to bring this into their hospitals.
Antonia 36:15
Well, I think I would be exuberant too in that time if there was no laparoscopy and suddenly there was. It’s such an Important innovation. But then I see where this is going, where people started getting hurt, right yeah right.
Howard 36:30
A lot just meant a lot of inexperienced Docs were sticking these needles through the belly buttons and then piercing things like the aorta and other Things you should stick needles into, because they didn’t understand the correct way to place the needles or the trocar and what the angles were that should be used to avoid Injury and especially what to do when things were difficult. If you had a hard time establishing insufflation, what do you do? So there were injuries, there were deaths from tubal legations and there was a huge backlash. And then there was this great hesitancy even in gynecology about laparoscopy and a lot of physicians around the country became criticized for doing something so risky.
Antonia 37:11
And is this where the Hassan technique came to the rescue.
Howard 37:14
Right. So the needle, the varus needle, was the big issue here and it was causing major vascular injuries which were significantly harming and killing patients, as I said. So Hassan, also a gynecologist, developed this open entry technique. That was a solution to that problem at least, and, in fairness, some of the injuries were also due to poor visualization and some of them were due to bowel injuries from coterie Like. The equipment was not great back then and you were looking down this scope with your eyeball Because there was no video laparoscopy. But the Hassan technique promised to fix the problem at least a vascular injuries that were the most ominous and lethal one. So Herith Hassan, as I said, a gynecologist, developed this in 1971 in the face of seeing vascular injuries and all the criticism of laparoscopic procedures, and so his technique eventually became the answer to the criticism and they could say well, we changed to this new thing and so everything’s going to be okay so after the initial exuberance, surgeons in hospitals and other people really swung back to Condemning laparoscopy right definitely in.
38:19
For example, Kurt – and this was international, Kurt Simon in 1983 Did the first laparoscopic appendectomy and he was actually condemned by the German board of surgery for being so lucky and brave. Another German named Eric Moret did the first laparoscopic cholecystectomy and after he presented his report in 1986 he was condemned and actually got into serious legal trouble in Germany.
Antonia 38:41
Gosh, that’s the year I was born. That’s crazy oh and, but didn’t they have good outcomes?
Howard 38:46
Yeah, yeah. This was happening, despite good outcomes was happening all over the place. In the United States Cameron Najat, a Gynecologist, pioneered and invented video laparoscopy and nearly lost his medical license over it. Part of this was heat coming from general surgeons who were staying 10 miles away from laparoscopy during this time period and, of course, if there was a vascular or bowel injury Then the generals or the vasculars had to come get involved and save the Gyns’ butt. So they were quick to condemn the gynecologists who were doing these things, and so a great conservatism Crept over a laparoscopy and it took until the late 1980s, really, for that to move forward interesting.
Antonia 39:25
So by the 1980s, when Laparoscopy was regaining ground again, there was a renewed exuberance at South, and this included gynecologists who embraced the varus needle technique for entry and insufflation. And this was in people mainly who had been already using it for probably 10 years or more and felt like they could do it safely, and then they were defensive when other surgeons attacked them for using it. So Early trailblazers like step, toe or polymer use the varus needle.
39:57
Yeah. So because these early trailblazers, like step, toe or polymer, use the varus needle, a lot Other gyne surgeons looked up to them and followed suit and continued to use it themselves and defend it. But then there were also these younger gynecologists and otherwise more moderate, risk averse Surgeons who would primarily use the Hassan technique because they felt like that was the salvation of laparoscopy and made it much safer. So then when general surgeons finally started using laparoscopy, they tended towards the Hassan entry because they had had two decades of criticizing the varus needle. So what about direct entry?
Howard 40:40
Well, blind direct entry no, no camera, just literally a metal thing you shove in the abdomen had been described but was not really popular at all during this time. And of course, optical direct entry, like many of us use today, was still a couple decades away because those trocars didn’t exist and hadn’t been developed. But I will say that the Hassan technique wasn’t just viewed as a salvation for decreasing the risk of vascular injury, but the folks again, primarily general surgeons who believed in it and some gynecologists obviously, who embraced it, they believed it also prevented bowel injuries. But that’s definitely not true. It eliminated vascular injuries but it actually, if anything, increased the risk of bowel injuries.
Antonia 41:21
Well, let’s get into data that compares the different methods. So again, 50% of all complications of laparoscopy occur with the initial puncture. So it’s critical to pick the safest methods and the safest anatomical locations.
Howard 41:36
Yeah, and that includes robotic surgery as well. Right, you still have to put a trocar in the belly, whether it’s traditional laparoscopy or robotics. So this question is very difficult to answer from data and literature because, well, fortunately complications are fairly rare and the types of patients and pathologies and other complicating factors are so varied that the best answer to this question can’t easily be gained through a large randomized control trial. No, no trial would be large enough essentially to figure this out, account for all the variables involved. So we have to look into the murkier shark infested waters of interpreting retrospective databases which, as we discussed a couple of episodes ago, is difficult because it’s just hard to control for Unknown variables and the complexity of patients and things like that. But it’s our best effort at this at least.
Antonia 42:25
Yeah. So the data on what’s the best laparoscopic entry approach is heterogeneous. At best, there’s a lot of systematic reviews that try to pull data from multiple studies, but even most of those are too small to find differences in those rare events. But still we can make some at least some comments from these studies, and they tend to favor direct entry over the other methods. So, for example, there was a systematic review published in 2021 that found that using the Varus needle was associated with increased incidence of extraperitoneal insufflation, omental injury, failed entry and trocar site infection. This review had just over 3000 patients total. It combined several different studies and even that number is still too small to capture a true difference in the rates of bowel or vascular injury. But even without that review, or even if these outcomes were the same, the data still appears to favor direct entry.
Howard 43:29
Yeah, and that’s a problem with reviews of randomized controlled trials, that there’s just not that many patients in them. The current Cochrane review pulls data from 57 RCTs and there are still only 9,865 participants, so we have to look beyond RCTs to answer this question. But even from the study you just mentioned, it’s clear that we should probably not be using the Veress needle.
43:51
And I think that’s one of the lessons from this historical tidbit that the gynecologists clung to this too long due to maybe an inappropriate emotional attachment to that needle, because they’d found themselves defending it against general surgeons who were criticizing it. On the other hand, general surgeons were happy to never use it. They embraced the open technique. But I think that we’ll find that both of these approaches are wrong and reactionary and both have an undue attachment to this argument between surgeons and gynecologists that lasted over a couple of decades.
Antonia 44:22
Well, both of those techniques are more old school because direct optical entry, which you could say is an improvement, wasn’t available or possible when laparoscopy first came around and then when it did become more common it had its own learning curve and I think it probably spooked people whenever there was a complication, especially during that learning curve. So direct optical entry really has had to fight against the old school habits and traditions of the varice and Hasan. And those are really strong forces and I’ll admit I was trained predominantly on varice entry. I did hundreds of them and I still love it irrationally.
45:03
Every time I do direct optical entry it still feels uneasy and I still remember I had one attending early on in my training explain why he would never use that direct optical entry.
45:16
He had watched a case in his own training where the optical trocar went straight through a major vessel and because it was bigger than the needle it made, a bigger tear caused that patient to have a catastrophic bleed and die on the table.
45:29
So I’ve had this highly deterrent, horrifying visual for this technique from a third-hand anecdote and I’m sure many other trainees at least from this attending heard that same story and then developed that same aversion to direct entry. But the review I just mentioned earlier does say, for example, that there’s that increased incidence of extra perineal insulation and failed laparoscopy with Veress. And I’ve had my fair share of pre-perineal insufflations and it’s very annoying and it probably makes my love for the Veress needle even more irrational, because we know that most serious complications, like the bowel or vascular injuries, develop after pre-peritoneal insufflation, because that just makes every subsequent attempt harder and more risky and it’s the Veress needle specifically that predisposes to those issues more than any other technique. So for all the Veress lovers out there, including myself, we really just have to make ourselves unusually every time we do surgery if we want to follow best practices.
Howard 46:35
Well, that’s all a great example of how we do adopt practices well beyond surgery, based upon emotional tenor and cognitive bias, and it’s hard to overcome these examples in our minds or our own experiences. If we’ve had everything always go right with one way and we’ve had a problem or two with another way in our careers, we’ll tend to favor the former over the latter, even if the literature says that that’s backwards from reality. So it’s a good lesson on how we have to remain emotionally detached when we interpret scientific literature. But, as you said, this technique the Veress needle, and Hassan for that matter is mostly used by older gynecologists and older surgeons who were themselves mentored, as you were, by charismatic older gynecologists, and we have to work on abandoning it.
47:27
I guess One of the few places where the Veress needle might still have a use is in morbidly obese patients, when it’s used through the uterus. So this is a technique that a lot of people don’t realize is available to them. But you can stick the long Veress needle either in the posterior cul-de-sac or all the way through the uterus, as if you were intentionally perforating the uterus with the uterine sound, and then insufflate the abdomen by that route, and this can be very helpful for a patient who’s morbidly obese or that has failed. Some approaches abdominally through the umbilicus, just difficult to get in. You’ve had pre-peritoneal insufflation and I’ll admit I also will put a needle in an umbilicus occasionally when I’m doing a post-hysterectomy vaginal vault surgery where I open the cuff back up and I’m just having a difficult time identifying the peritoneum and I can stick a needle in her belly button and insufflate the abdomen and see that peritoneal reflection. So I’m not saying I never use them.
48:17
Well, I had never thought of insufflating by perfing the uterus with a Veress, but yeah, it’s a great technique for super morbid, obese patients, especially if you’re having difficulty with those long trocars and elevating the abdominal wall. So it’s a good trick to remember Now, just as gynecologists have held on to the Veress needle for a long time, in the same way, as I said, I think the general surgeons have persisted with the Hassan technique and generally misunderstood or overpromised its safety profile. It does indeed reduce the risk of vascular injury, but it increases the risk of bowel injury and I think that’s not generally understood among general surgeons. But that’s the sort of thing that’s hard to tease out of all this retrospective population level literature.
Antonia 48:59
You mean what you were calling the murky shark-infested waters of retrospective databases? Is there a kraken in those waters?
Howard 49:08
You just don’t. You don’t like my metaphors at all, but yeah, so let’s talk about some of these krakens. I’ll put a link to the kraken review that we mentioned for 2019, and one of the failures of kraken reviews like that one is that they again tend to only use prospective RCTs. So questions like this don’t have enough of those, and so they don’t really fairly represent these problems that can’t be fairly studied through RCTs. So the kraken review concludes with that limited data, that there’s insufficient data to recommend one method over the other. So again, we have to look beyond RCT. We can get an idea about the various injury rates by looking at some of the larger retrospective studies that are available, and these are controlled studies.
49:49
There were three large studies published by Hassan himself, bonjer and Gary that were done well before the availability of direct entry methods. But these non-randomized trials compare the rates of visceral and vascular injury between the open technique, or what we’re calling the Hassan technique, and then the closed technique, which to them meant using the varus needle for pre-insulflation. They still give us a good idea about the baseline rates of injury and, importantly, there were no vascular injuries in any of those studies, which together had over a million patients using the open or Hassan technique. But the varus needle was associated with a rate of vascular injury that was between 200 and.2%. So quite a range in those studies. Still again, relatively luckily it’s a rare complication. But for visceral injuries like to the bowel the inverse was true, with either no difference in visceral injury rate or maybe a bit higher visceral injury rate, especially in the Gary study when the Hassan technique was used. So it was as high as a half a percent in the Gary study compared to.04% for the varus needle.
Antonia 50:58
So the Hassan is definitely safer for minimizing vascular injuries but perhaps more dangerous in terms of bowel or visceral injury. But I thought it was also interesting in Hassan’s data that the complication rate for general surgeons using varus was significantly higher than the rate for OBGYNs using the varus.
Howard 51:19
Yeah, and I think that makes sense if you understand the history of it.
51:22
Again, a lot of variation to account for and types of surgeries and things like that.
51:26
But I do think that it demonstrates one of the fundamental differences between gynecologists doing laparoscopy and general surgeons doing laparoscopy. We naturally emphasize sticking whatever it is we’re going to stick in the patient through the umbilicus, whether that’s the varus needle or a direct entry trocar towards the uterus and therefore away from the bifurcation of the aorta and away from any potential lateral injury that might happen, for example to the iliacs. We have greatly emphasized the importance of the angle of entry and how the patient’s positioned. General surgeons, on the other hand, they still have a tendency to insert their trocars towards the organ they’re interested in, whether that’s the appendix or the gallbladder, and that necessarily means that the needle of the trocar is angled towards a major vessel. In fact, I have a family member who went in for a routine appendectomy and ended up with a right-sided iliac injury that required extreme measures to save his life. So the nature of gynecology, I think, has predisposed our thought processes towards putting these trocars or the needle into a safer space, and we can talk more about that in a second.
Antonia 52:31
So you’re saying it’s a subconscious thing and general surgeons should try to think more like gynecologists and aim for the uterus to minimize.
Howard 52:40
They definitely should try to be more like us. Yes, interesting Cue the hate mail.
Antonia 52:44
Okay, so you think that angle of entry with the varus applies to direct entry or optical entry as well?
Howard 52:52
It definitely does.
52:54
There’s still less data on direct entry because it’s newer, but several retrospective studies do look at this technique and most of the direct entry data that’s been published is not optical entry but literally just a blind take-a-tro-car and blindly stick it through the umbilicus.
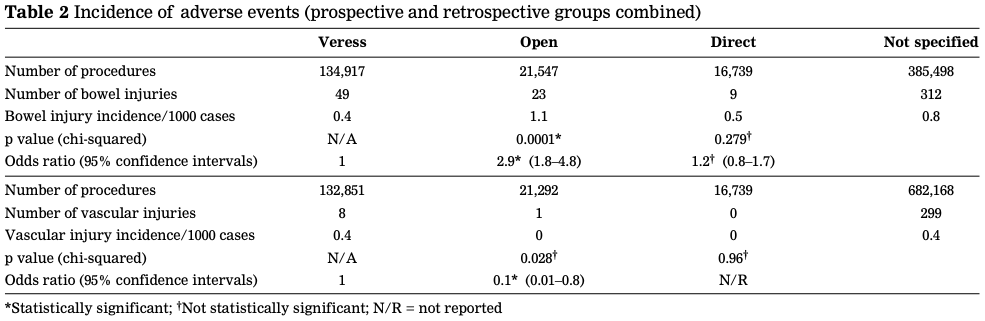
53:09
The prospective randomized trials in particular from the 1990s didn’t have optical entry available. These were by Borgata, Nezhat and Byron, but they were prospective randomized trials, unfortunately, though really not with enough patience in them to give us a fair answer to this. But if we summarize these data of just blind direct entry and compare that to the varus or Hassan technique from all of these various studies, the best answer we get is this Bowel injuries occur in 0.4 patients per 1,000 with a varus needle, compared to 1.1 per 1,000 with the Hassan method, compared to 0.5 per 1,000 with direct entry cases. So about the same between varus and direct entry, but almost double with the Hassan for bowel entries. And vascular injuries occur again in 0.4 per 1,000 varus needle cases that was a varus needle at my family member’s surgery compared to zero vascular injuries per 1,000 in either open or direct entry methods.
Antonia 54:16
That’s really interesting. One would think that blind direct entry would be the worst, because you’re jamming a larger, wider, sharp tool into the abdomen without seeing what you’re doing. So I think it really says a lot that even that still has less complications overall.
Howard 54:34
You’re still, with a varus needle though, directing this blindly into the abdomen.
Antonia 54:38
Yeah.
Howard 54:39
So it’s all about the angles.
Antonia 54:40
Yeah Well, this comparison. It wasn’t completely equal, because there was 130,000 cases of varus compared to 20,000 with Hassan and even fewer with the blind direct entry. And then you have to wonder, because this is combined right Prospective, retrospective Does this include some selection bias based on complexity or other factors? Because maybe someone might tend to favor the Hassan method for someone that has multiple prior surgeries and lots of potential adhesions and then favor direct or yeah, direct or various for their less complex patients. So it’s hard to say that that I mean, this isn’t exactly perfect data, of course, but if all things were equal, then I think the conclusion from that comparison would be that the virus really has to go and it seems like the direct entry is king.
Howard 55:38
Well, you’re right, though. It is combining perspective and retrospective data to get these numbers. Some of them did control for case complexity, some of them didn’t, so lots of potential limitations here. Sharks krackens indeed in the water, but remember this is about blind direct entry, not optical direct entry which we would use today.
Antonia 55:58
Yeah. So we’ll have to extrapolate a little here, but in theory at least, the optical direct entry, where we can see the layers as we pierce through them, should make this much safer than the blind direct entry. Even if we just put the camera straight into a bowel or even a major vessel, at least then we would be theoretically identifying it early on, and that’s better than an unidentified entry. So if it’s true that by seeing where you’re going through, as you’re going through it, that it’s safer, then the numbers would look much better with similar data today comparing optical direct versus virus versus Hassan entry. So we still can’t say that for sure, but based on everything that we know so far, it does seem that direct optical entry really probably is the safest and we all really should just feel better about using it and we should opt for it. So let’s move on to talking about where to place this first trocar.
Howard 57:01
Well, for the sake of time, let’s simplify that down to either talking about placing it around the umbilicus or around what people call Palmer’s Point, because I think that those are the two primary places that gynecologists are placing these trocars today. So maybe let’s talk about umbilical placement first. Now, you pointed out that there are different places. When you say umbilical, it could be in different places.
Antonia 57:22
Yeah, some people put it just below or just above versus right inside the belly button.
Howard 57:29
Yeah, and I think the principle here is to understand how the tissues of the abdominal wall view transversely, how they relate to the angle of trocar entry. So the whole benefit of using the umbilicus as an entry point is that the base of the umbilicus represents the thinnest part of the abdominal wall, even in obese patients. So you want to be in the umbilicus, not below it or above it when you stick a trocar in at an angle. If you do that at the base of the umbilicus, you’re still traversing a relatively short distance. But if you’re below the umbilicus and you stick it in at the same angle, particularly if the patient is obese, you may not have enough trocar length to get into the abdomen. So it makes a huge difference as the patient’s abdominal wall gets thicker with obesity.
Antonia 58:13
Yeah, just think about how much you have to skype through and you’re going through the skin that’s outside of the belly button. Maybe we can find a good link to just the visual graph of that. Yeah, because that distance of sub-queue tissue really can be a deal breaker in some cases. I think the reason people would still do that is that they’re worried about closing skin. That’s deep inside the belly button and it’s harder to access with a stitch compared to closing skin anywhere else on the abdomen. But if you’re not doing the Hassan technique where you need a relatively large incision, you really should be inside the umbilicus as often as possible.
Howard 58:55
Yeah, if you’re using a one centimeter incision and you’re closing the fascia or bigger for the Hassan method and you’re doing a sub-cuticular in the skin, well all that’s going to become very difficult if you’re in the base of the umbilicus. But if you’re using a five millimeter trocar and you’re closing the skin with glue, which is what you should be doing, then you don’t have any concern at all about the difficulty of closing that umbilical port.
Antonia 59:17
Okay, so we’re favoring the inside, the deepest part of the belly button, for entry and then, when you’re actually inserting it, the angle is everything. As you mentioned, the gynecologists are taught and they just intuitively will aim towards the uterus, which puts at an angle away from the aorta and also keeps the trocar tip central and midline to avoid the iliacs.
Howard 59:43
Right, and this will vary a little bit by how heavy the patient is. I encourage my students to put their finger in the umbilicus and press down and fill the pulsating aorta beneath it. It’s important to appreciate how close we are to the worst possible injury you could cause. So we need to angle away from that. In a very thin patient, you want to elevate the abdominal wall and have a greater than 45 degree angle directed down into the pelvis to avoid the aorta. In a patient who’s overweight, this angle might decrease to 30 to 45 degrees. And in a very obese patient, where the abdominal wall tends to drape down and fall when you elevate it up, at least you may only need a zero degree angle. Elevation of the abdominal wall is key and elevation takes care of most of this problem when you elevate below the umbilicus, pulling it upwards. But you can’t do this with a very thin patient, so you have to have that 45 degree angle to avoid the aorta.
Antonia 01:00:35
Yeah, and if you overshoot it, especially on an obese patient, and you angle too far down, then it just means you don’t get in, You’ll be driving through out of posity. But you can try again and reduce your angle.
Howard 01:00:48
Right, and if you’ve insufflated before you do that, it’s going to get tougher because the peritoneum is pushed away.
01:00:53
So that’s what we call filled laparoscopy. So the angle becomes more obtuse the more obese the patient becomes. And it’s also important to learn the layers of tissue that you see, so that you can be cognizant of any problems with adhesions or potential bowel injuries you place at trocar, or even just how hard to press at different layers. So that’s what the optical trocar allows you to do, and so you see first the subcutaneous fat, followed by the fascia and muscle, and then preperitoneal fat and then finally the peritoneum, and you should become really good at identifying those layers.
Antonia 01:01:24
Okay, so that’s the umbilicus. What about Palmer’s point? I think it’s maybe regained popularity, partly because it’s part of the standard in robotics. A lot of robotic assisted hysterectomies encourage the first trocar to be placed at Palmer’s point, or at least yeah, at least the initial insufflation. It allows the instruments to be higher up, which is more optimal for the mechanics of using the robot for hysterectomy, and it also often avoids scar tissue in patients who have had at least certain types of prior surgeries, because usually they haven’t had surgeries in the left upper quadrant before. I mean, that’s not always the case, but usually.
Howard 01:02:03
Yeah. Yeah, the traditional four or five port robotic approach often does start with a Palmer’s point insertion. But here again it’s important to understand what it is that’s actually safer about Palmer’s point and when it should and should not be used. Palmer, who was a gynecologist we can tell the surgeons that and they’ll stop doing it had identified that this point, which is described as the being at the mid-clavicular line about three centimeters below the left costal margin, was associated with the fewest adhesions, as observed on autopsy specimens. But this was done prior to the advent of things like gastric bypass surgery, if you think about it. The appendectomies and the cholecysterctomies they all took over the right side of the abdominal wall. And then the pelvic inflammatory diseases and other pelvic surgeries or C-sections. They took over the pelvis. So what you were left with was the left side. But that was true in Palmer’s day, but not necessarily true today.
Antonia 01:02:56
Yeah, because we don’t favor this in people who have had a splenectomy or stomach surgeries, especially bariatric surgery. But it’s typically reserved for patients who have known or suspected adhesions in the pelvis, maybe a prior midline vertical incision or multiple prior umbilical punctures from prior laparoscopies, and it’s still appropriate if you’re worried about abdominal adhesions. So the question is, should we use it in every patient or just select patients?
Howard 01:03:25
Exactly, and today we have the ability to use ultrasound to identify abdominal wall adhesions. For patients with those prior surgeries that you mentioned, this strategy is still underutilized so we can’t just say routinely if you’ve had three or more previous umbilical trocars then you should always use Palmer’s points. But today we can be more precise and we can say we should do an ultrasound to map the adhesions by looking at the visceral slide under the umbilicusand then make a decision about whether to use that or go to a different place. So I would limit it’s use to patients who have ultrasound documented adhesions and, like the openness entry technique of his son, we have conflated Palmer’s point entry as being safer, because it’s safer for adhesions is also being safer to prevent vascular injuries.
Antonia 01:04:11
Yeah, it’s easy to mix up, but there isn’t actually data saying there’s a lower vascular injury risk with Palmer’s.
Howard 01:04:19
Yeah, it was all about adhesions of bowel and vascular injury is, frankly, much worse than visceral injury. The trocar is still very close to the aorta, even with Palmer’s point. When you think about how far you are off to the side, particularly in thin patients, there’s not a lot of distance there and I’ll note that modern image based analysis of where adhesions are likely to form not the autopsies of Palmer’s days but MRIs and CT scans of today would tell us that Palmer’s point needs to move down a little bit roughly to the level of the embolicus, but still in that left mid-clavicular line and if I need to make an alternate entry, I use ultrasound to understand where my safe place is.
Antonia 01:04:59
It’s also important to understand the layers of tissue that you’re expecting to penetrate through when you go through Palmer’s point, as opposed to around the umbilicus. So the optical trocar will pass through skin, then sub-Q fat, followed by external oblique aponeurosis, then internal oblique, then the transversalis muscles, then possibly some more extra peritoneal fat and then into the peritoneum. So there are three layers of muscle that you would penetrate to get through there. If you find yourself only going through two layers of muscle, then you’re too medial and you’re really putting the aorta at even higher risk.
Howard 01:05:38
Yeah, and the angle again is so critical, particularly on a thin patient who has a narrow chest wall, and the optical trocar gives you the advantage too of understanding that you’re in the correct place and then, more importantly I think, identifying complications if you see something abnormal. And this is more difficult, again, the thinner the patient is. Just as it is an umbilical laparoscopy, but there’s simply no evidence that Palmer’s point should be used routinely for every case or that doing so would decrease the rate of complications. We don’t have the large enough series of patients to understand how many vascular injuries are occurring with the use of Palmer’s point, just to use it.
Antonia 01:06:17
Okay, so it sounds like we should limit the use of Palmer’s point injury to those patients who actually have high risks of abdominal adhesions near the umbilicus, and we should also, when we do use it, consider moving further away from the costal margin. I don’t think we have time still left to talk about management of trocar injuries, but the most important thing there is identifying that they’ve occurred.
Howard 01:06:41
Yeah, exactly, and I think optical gives you that benefit or an advantage there. I also think, realizing that it, as you said, if you’ve had a pre-peritoneal insufflation, you’ve tried a couple of times and you’ve insulated and you’ve distended the peritoneal away from the abdominal wall, especially for that second or third or fourth attempt, that’s when an increasing number of these injuries occur, probably because people angle the trocar more and more straight down into the abdomen and then they find themselves at the aorta. So you should really consider doing something different if you fail twice to gain peritoneal insufflation.
Antonia 01:07:14
Yeah, maybe we’ll just end with saying that we’ll put some links to some review articles that our listeners can read about how to manage vascular injuries in particular. This is an emergency, so there has to be an emergency protocol, just like there would be for postpartum hemorrhage or shoulder dystocia or something else high acuity and life threatening like that and in those scenarios seconds matter, but I think we really are out of time for.
Howard 01:07:40
Another unintended consequence of Supreme Court of Alabama is that we can’t talk about complications management in this episode.
Antonia 01:07:47
Yeah, shame on them.
Howard 01:07:49
Those guys.
Antonia 01:07:50
Okay, well, the Thinking About OBGYN website will have links to things we’ve just discussed today and we’re going to be back again in a couple weeks.
