
Episode 8.12 Four Tips for Paps, OB Unit Closures, and the Importance of Hospital Based Obstetrics
In this episode, we give four simple tips for performing a Pap smear. Then we dive into the complicated problem of obstetric units closing across the United States and actions we need to take to stop this dangerous trend that threatens the safety of pregnant women and newborns. Also, we highlight the important of hospital based obstetric programs and the history of why births moved into the hospitals in the beginning of the 20th Century and the 99% decline in maternal and neonatal mortality that followed.
00:00:02 Cervical Cancer Screening Tips
00:14:13 Hospital Closures Affect Obstetric Care
00:37:27 Rural Obstetric Units Closing Challenges
00:44:53 Hospital vs. Home Birth Safety
00:49:40 Healthcare Disparities for Women and Children
00:55:08 Evolving Birth Settings in America
01:02:28 Email Advocacy for Healthcare Reform
Links Discussed
What Is the Best Collection Device for Screening Cervical Smears?
FDA Approves HPV Tests That Allow for Self-Collection in a Health Care Setting
Obstetric Care Access at Rural and Urban Hospitals in the United States
As hospitals close obstetric units, maternity care deserts become more common
Federal plans to reduce maternal mortality draw praise and some criticism
How to Prevent Rural Hospital Closures
Why Are Obstetric Units in Rural Hospitals Closing Their Doors?
Legislative Milestones in Medicaid and CHIP Coverage of Pregnant Women
Medicaid reimbursement, prenatal care and infant health
Transcript
Announcer: 0:02
This is Thinking About OB-GYN with your hosts Antonia Roberts and Howard Herrell.
Antonia: 0:18
Howard.
Howard: 0:19
Antonia.
Antonia: 0:20
What are we thinking about on today’s episode?
Howard: 0:22
Well, we’re going to talk about the crisis that’s been leading to the closure of birthing hospitals and birthing units all across the country, especially in rural areas. But first we have four tips for performing a pap smear.
Antonia: 0:36
Well, pap smears are really bread and butter for gynecologists, and our listeners might be surprised that we would even have four tips for something that’s so basic. But I bet there’s actually a lot of variety in the way different providers do pap smears or, more properly, collect cytology for a cervical cancer screening, because we don’t technically do pap smears anymore. We do liquid-based cytology with HPV as indicated for cervical cancer screening, cytology with HPV as indicated for cervical cancer screening. And even that model might be going away soon because in the foreseeable future we may be predominantly just doing primary HPV screening. The American Cancer Society already recommends that now, and that would start at age 25 and just be repeated every five years. But then that would also need to reflex to cytology if there’s an abnormality. So, regardless, it’s important that we collect these specimens correctly. So let’s talk about it.
Howard: 1:33
Yeah, and I also think there’s a lot of variety in the way we do this because, frankly, there’s a lot of myths about the collection of PAPs. We don’t have time to talk about all those, but it’s also something that no one really discusses formally. When you’re training, if you’re a med student or an intern or a resident well, it’s just assumed that you know how to do this and that you’ll perform it in a way that those around you you see them do it and perform it, and so without anybody ever really questioning all of the dogmas and myths and traditions and whether you can do it when they’re a patient’s honor period or things like that. So one of those is about the use of lubricants. So our first tip is that you can and should use lubricant when you do a pap smear.
Antonia: 2:16
Yeah, that’s a good starting point to clarify. Actually, there may be some confusion and misunderstanding about the belief that lubricant would somehow alter the pap specimen and maybe make it invalid or unreadable. But there’s no reason why you can’t use an appropriate lubricant when you collect a pap. The typical sterile lubricants we have in our clinics, or even commercial products, like Astroglide, for example, don’t contain any substances that would interfere with the liquid-based PAPs. And even if you did use some kind of lubricant that did contain some kind of substance, really as long as you’re using a sparing amount on just the outside of the speculum, just so that it can be inserted without a whole bunch of friction and discomfort, then it’s not going to actually get into the pap result or affect it. So there’s just no reason not to use a lubricant when you’re inserting a speculum. This may have been true once upon a time that it would have messed up the pap smears, but times have changed. So if you use it judiciously now, it’s just not an issue.
Howard: 3:24
And prompt to ask other questions about like how much blood and things like that too. So a lot of the things that you hear about this are myths. Another big variation we might see is in the type of tool or swab that you use to collect the pap. So there’s a cervical broom that has the soft silicone type bristles on it, and there’s also a cervical spatula with two different shaped ends one for the cervix and the other for a vaginal cuff, and then a cytobrush. It’s like a pipe cleaner or a mascara brush. I don’t use mascara.
Howard: 3:54
So, for the listeners to know. Antonia had to tell me it was like a mascara brush. But we’ll frequently see any of these types of brushes, the three of these, or see them used in different combinations used to collect the specimen.
Antonia: 4:07
Yeah, I’ve seen all of these, but most commonly I’ve really only had available the spatula and the Cyto brush, and that’s how I was trained to. For whatever reason that, the broom is not as often available to me, and I think it’s a shame because it’s probably the least uncomfortable with its soft bristles and the fact that you only need to use that one thing and not two things. So our second tip is use the broom only instead of the spatula or the cyto brush or the combination, if at all possible.
Howard: 4:42
This one’s confusing when you try to read studies about which one you should use. There are lots of studies that have been published over many, many years and from many different countries, and that’s a point of confusion. Sometimes, too, that will compare the quality of the collected specimen, depending upon which of these instruments you might use to collect them or in what order you might use them. But you have to be careful in reading these, because many of the studies that have been published are about conventional pap smears where for decades the air spatula was used wooden or plastic, and the original ones were wooden. And then over time you still get them distributed to gynecology offices now in a plastic version.
Howard: 5:23
But the broom has been shown to be superior to the spatula, so there’s really not a reason to use a spatula.
Howard: 5:29
But I think again, like we’ve just ordered the spatulas for years it’s what we used to use, and back in the days of a conventional pap smear.
Howard: 5:37
But the broom is what’s recommended in the FDA approved protocol for liquid-based cytology and it doesn’t require that you use the Cytobrush in the FDA approval in the original studies in addition to the broom. But you might use it in select cases, especially if the transformation zone is not easily seen. That’s the thought of that, but there’s no evidence that routinely adding the Cytobrush enhances patient outcomes meaning cervical cancer dysplasia detection compared to using the broom alone. There are a couple of studies that show that if you use a Cytobrush in addition to the broom, that it doesn’t help you acquire any more into cervical cells, which I think would be the thought of using the Cytobrush. There are also some studies that do show the opposite, when you just look at like total cell count and things like that, but there aren’t studies that show that patient outcomes are specifically made better when you add the Cytobrush to the broom. So use the broom over the spatula and the Cytobrush doesn’t need to at least routinely be used in addition to the broom.
Antonia: 6:34
Yeah, if you just physically look at these three different tools or look at pictures of them, you can see how the broom would combine the best of both worlds of the spatula with its kind of broader lateral reach to get ectocervical cells, and the cyto brush which kind of gets more internal endocervical sampling. And of course, like we said, the broom is more comfortable because it’s softer. The only downside I can think of with having primarily just brooms available is that if you were doing a colposcopy with endocervical curatage, you can’t get that with a broom. You still have to use a cyto brush or some other tool for the endocervical curatage. And of course they are the more expensive of these tools which we’re talking about just single digits of dollars per thing. But you know, I suppose that could add up.
Howard: 7:29
Yeah, and I use it, just like you said, the Cytobrush during that procedure as well, and I have all three in my office. So it’s a choice for me. I realize it’s not always for some folks. We should review again sometime whether routine ECC is necessary during every colposcopy, maybe when we get Stuart on the podcast again. That was in his belly wick. But despite being more expensive, the brooms are still more cost effective than spatulas alone due to their superior collection. So there was a decision analysis study in South Africa where the cost of spatulas was two cents and the side of broom there was like 22 cents, and due to the improved detection that the broom afforded, it still was found to overall be more cost effective. They unfortunately didn’t factor in the scenario of using this cyto brush plus spatula, though.
Antonia: 8:14
Yeah, and, as you said, there’s been different studies from different countries about this and from what I’ve seen, if we’re looking at costs now in the US that it looks like cyto brushes maybe cost about one-fourth of what the cyto broom would cost. So, for example, it would $1 a piece instead of $4 a piece or something like that. So, yes, the upfront costs of using a spatula even a spatula with a cyto brush is still going to be cheaper front than using the cyto broom. Let’s say it might cost half. And there are other studies that compare this combination to the broom alone. And maybe there’s conflicting results again because they’re from different countries or they’re looking at pap smears instead of cytology. But even if the detection rate was the same, even if it wasn’t superior technically which it is but even if it wasn’t, I wonder if just the difference in how uncomfortable the spatula and cytobrush are could actually affect people’s compliance in getting follow-up PAPs and maybe cause people to even avoid or miss screenings because of how uncomfortable their last PAP was.
Howard: 9:26
Yeah, and a lot of this literature is confusing because it looks at not liquid-based cytology but slides. So when you’re looking at stuff that’s from a foreign country or stuff from the US that’s more than 20 years old. You may be confused by that, but that’s a reasonable speculation, something hard to prove or disprove. But think about some of the other things that we advocate for solely to improve patient comfort, even though they might cost a little bit more, we’re talking a few cents here.
Antonia: 9:52
Probably, yeah, and we should. If it’s more comfortable, well, and it’s superior, we should do it if we can. So here’s a free research idea for someone out there that’s looking for ideas so you could randomize routine pap patients to either a spatula and cyto brush or a cyto broom and then do a survey on their experience, like how painful was that? How likely are you to come back and get that again if you need another one?
Antonia: 10:17
But besides these three tools, there’s been all kinds of other ways paps have been collected that have been described, even Q-tips or tampons, and even tampons actually, the specimens seem to be quite adequate, surprisingly so. And of course now we know there’s some FDA-approved self-collection kits for checking cervical HPV that I’m at least, very eagerly waiting to become mainstream. So anyway, I suppose if there’s an important reason you definitely want to get the endocervical cells, then you need to have some cytobrushes on hand for that. But it may be unnecessary for just the routine low risk screening. So anyway, on to the third tip, and that is when you’re using this broom. Rotate it five times in the same direction. You’ve got your sample.
Howard: 11:05
Yeah, and that sounds so basic, but I honestly think a lot of folks don’t do it that way. So it’s five complete rotations in the same direction, so that the cells are being gathered up on the instrument, rather than twirling it back and forth in your fingers, maybe knocking cells off that you collected, or perhaps just not making a complete 360 degree rotation, because you’re swiveling in an arc less than 360 degrees. So five times in the same basic direction and depending on which product you use, you may or may not have to take the brush head off. So if you use the SurePath product, then you pop the head off of the brush and leave it in the container, but if you use the ThinPrep product, then you push the brush against the bottom of the container and then swirl it vigorously and then throw it away.
Antonia: 11:48
Yeah, that five rotations thing. That might be another thing that makes the broom superior in specimen collection, because with how rigid the spatula is it can be hard to even rotate it around once for someone who has maybe an atrophic vagina, atrophic cervix, and it would actually be hard to do that. So that probably leads to less adequate specimens. Anyway, let’s get to our fourth tip, and that’s just, that’s the implied giveaway. Just follow the PAP guidelines, like we say so often. So in the US that would be the ASCCP and that’s endorsed by ACOG or just whatever your correspondent national society guidelines are. If you’re outside the US and it sounds so obvious, but at least in the US we know that many women are still not really having pap smears done according to the widely accepted and validated guidelines.
Howard: 12:47
Yeah, and we certainly don’t have to beat a dead bush over this.
Antonia: 12:51
Mean a dead horse.
Howard: 12:52
Yeah, a dead horse.
Antonia: 12:53
Oh, you made a malephor there.
Howard: 12:55
A malephor?
Antonia: 12:57
Yeah, where you mix two metaphors together the wrong way, like don’t burn your bridge at both ends, or something like that.
Howard: 13:06
Oh, okay, yeah. Well, I think for this we’ve just scratched the tip of the iceberg.
Howard: 13:11
Yep Very good yeah, but I do think it’s interesting how simple all these things seemingly they are. They’re simple things, yet they’re not always done correctly and there’s a wide variation in practice, despite fairly clear cut and evidence-based recommendations. I do think that’s just because, for a lot of these things, especially simple, routine things, the everyday things that seem simple to us we just do whatever the folks around us do and our practice is informed by the local culture rather than scientific evidence.
Antonia: 13:40
Yeah, once we’ve been taught to do things a certain way, especially when we’re early in learning and we’re just dying to learn how to do it so I can do it myself, it becomes an ingrained habit and then we’re just uncomfortable changing away from those established practices.
Howard: 13:56
Yeah, well, let’s move on. There’s a new report in JAMA from December 4th that looks at obstetric care access in rural and urban hospitals in the United States and the changes between 2010 and 2022. In that time period, 537 hospitals lost obstetric services throughout the United States. Now there was some new openings of units, but only 138 units were opened in that same time that 537 were closed, so the net effect is a loss of 399 birthing units over that 12-year time period. By the end of 2022, there were 2,705 hospitals in the United States with obstetric services and another 1,934 hospitals without obstetric services.
Antonia: 14:41
Right. So that’s out of total hospitals in the US, but these losses are affecting rural hospitals much more profoundly than they are urban hospitals. 238 of the hospitals that lost OB care were considered rural, and only 26 of the new units with new OB units were opened in rural areas. So that’s a loss of over 200 L&D units in rural USA. 112 of the new units were opened in urban areas and the losses as a percentage were much less in those settings. So by the end of 2022, 52% of rural hospitals did not offer OB care, compared to just 35% of urban hospitals.
Howard: 15:32
And the impacts of closing in a rural area versus an urban area are usually different, although not always, but in most cases, if a rural unit closes, that was the only place in that area where women could go for obstetric services, whereas if an urban unit closes, well, there’s usually other units in the same city that are able to absorb the capacity that was lost. Many cities have several obstetric units within a few miles of each other, whereas in a rural situation, if a rural unit closes, the next birthing hospital might be more than an hour away, in some cases, much further.
Antonia: 16:09
Yeah, and you have to think it’s not just the obstetric services that get affected by that. So if you think about a generalist full scope OBGYN suddenly being told sorry, we’re going to shut your LND down at the end of the year, maybe some of those doctors will stay put and just continue practicing gyn only. Maybe they’ll try to, every once in a while, go moonlight somewhere over an hour away. Maybe they’ll continue to see office OB patients and then at third trimester, say, okay, now you need to go establish at that other hospital that takes you two hours to drive to because that’s where you’re going to deliver but there and there’s a lot of drawbacks to that I see that happening.
Antonia: 16:51
But for the most part, a lot of those generalist full scope providers are probably going to want to pack up and move someplace where they can continue what they were trained to do of delivering babies. So this means that in that case the hospital may lose most or all of their gynecology services as well. And so not only is it that women can’t just deliver babies at that hospital, if someone shows up with an ectopic pregnancy or they’re hemorrhaging from maybe a miscarriage or something or some other kind of gynecologic emergency, they’re going to be in trouble. There’s going to be nobody to help them. So it’s really a loss of access to all of women’s health services, since the labor and delivery unit is essentially a centerpiece of most OBGYN practices.
Howard: 17:42
Right, centerpiece of most OBGYN practices, right, and there’s no good evidence that this closing of hospitals has closed since the end of 2022, when this study terminates.
Howard: 17:52
The environment that has been accelerating the loss of these units over those many years has only worsened.
Howard: 17:58
There was a little surge of closures during the COVID pandemic, because I think that the COVID pandemic for hospitals in general was a stress test for their financial and structural viability. If you were already struggling, covid may have pushed you over the edge, but there was a report in a journal called Chief Healthcare Executive from September of 2024 that said that an additional 100 hospitals nationwide have closed their obstetric units since 2022. Now I think that that number includes this, encompassing 2022. So from the JAMA article, we see that there were 32 units closed in 2022 specifically, but that still would mean that, as of September 2024, they were able to identify another 68 units 2023 and the first few months of 2024, that have closed their OB units, and now 35% of every county in the United States qualifies as a maternity care desert. According to the March of Dimes, over 1,100 counties don’t have a single obstetrician or birthing facility, which is a 10% increase in just the last two years since the previous March of Dimes report.
Antonia: 19:04
Yeah, that journal article also talks about things that are trying to be done to respond to that crisis. There’s a couple of things that came up that were mentioned. I’m not sure how helpful they’re ultimately going to be. One is the idea of having mobile units to provide prenatal care or things like increasing telehealth access. It seems like the urban consolidation response to the outlying rural counties is always something like don’t worry, your patients can call us on the phone and we can provide their prenatal care remotely.
Howard: 19:40
Yeah, which has some benefits. But if you think about the important parts of obstetric care, delivery of our obstetric system, almost all the real measurable benefit we provide to mothers and newborns comes during the delivery itself, not the prenatal period. There’s little compelling evidence that a lot of what we do in our structured prenatal visits has a whole lot of impact, but we save lives when patients with pregnancy complications show up at our hospitals. So creating mobile vans that listen to heart tones and measure fundal heights, things that aren’t necessarily even evidence-based, just doesn’t add a lot of value.
Antonia: 20:17
Yeah, we’ve talked before about what things are really essential that we do in pregnancy. So we give Rhogam to Rh negative mothers. That can’t really be done remotely. We accurately assign due dates. We use ultrasound for that. Maybe you could put a sonographer on a bus, or something I think it’s helpful to know is are you having one baby or two babies? But maybe that’s not the most vital information even there. And then, of course, we screen for hypertensive disorders, and measuring blood pressure is something that could be done remotely from home. People can get pretty cheap over-the-counter blood pressure cuffs or they could have one sent to them, and that’s an important screening tool for preeclampsia. And, as we’ve discussed before, it’s one of the reasons why we even have structured in-person prenatal visits is so we can bring people in and check their blood pressure a whole lot during the third trimester especially.
Antonia: 21:13
But more than telehealth and more than these mobile vans that may be able to do most of this stuff, really what we need is hospitals that deliver high quality obstetric care, and we need OBGYNs in those communities.
Antonia: 21:28
So the other thing that article mentions from the Chief Healthcare Executive Journal is a pledge from President Biden’s administration back in July 2024. So Vice President Kamala Harris had said, quote nearly every hospital in our country will soon be required to provide new mothers with delivery rooms that are fully stocked with life-saving medical equipment. End quote. And this was part of a CMS proposal to address minimum safety standards for obstetric services at hospitals, which apparently did not exist before. So these are now the standards, and obviously I think it’s a good start to at least have some standards at all, if there weren’t before. But I think the problem here, the elephant in the room, is that besides just setting standards and then equipping a unit, you have to staff it. And how do you do that if the OBs and nurses and midwives and anesthesiologists, et cetera, don’t want to work there and live there?
Howard: 22:32
Yeah, I’m not too optimistic about this yet. This stuff is difficult to fix, and when you talk to politicians and get politicians involved, they look for things to do in good spirit that are unfortunately budget neutral, and so we do have to spend some real dollars to fix this. They basically list a few suggestions of OB emergency resources and equipment to have on things like blood and fetal dopplers and nurse call buttons and things like that that I would. Even though it might not have been written on a list, I think that our emergency rooms and units are already doing so. I’m not sure that that means that there are OB units out there without these resources it just may not have been written down and qualified but I want to see instead how they intend to solve the staffing crisis, which, as you said, is not just nurses, it’s anesthesia providers and it’s obstetric care providers.
Howard: 23:25
Of course, it’s always nice to solidify training for emergency room staff nurses and physicians and help them understand how to manage OB emergencies, but we’re already doing that really in every hospital that has an emergency room in the country, or at least they should be, and if they’re not, you know. I’ll link an article that quotes my friend, Lisa Satterfield, who works with ACOG National, who actually listed that, said that she believes this proposal would be counterproductive after analyzing it and, if anything, could weaken many of the arguments that we’ve been trying to make to hospitals and payers and other relevant entities about why we need to shore up our obstetric units, particularly the rural OB units. The American Hospital Association has also criticized this proposal for similar reasons that it ultimately may do more harm than good and make folks feel like we’re fixing a problem when we’ve not really addressed it.
Antonia: 24:16
Yeah, the delivery rooms and the life-saving equipment that they leave to fill in the blanks on there. Those are only part of what we need, because we need the teams who know how to use that equipment too and are experts and they’re trained on it. The CMS proposal does include a provision, or a suggestion at least, that any OB unit, even if it’s a single room, be supervised by somebody with OB experience, and they say that could be an obstetrician or a midwife or a nurse. So theoretically a hospital could just have one single room designated as a potential emergency birthing suite. Maybe it’s in the ER, maybe it has a crash cart and a fetal Doppler available to the ER docs and nurses to use as needed. I would think ideally it would have a full kit for, like, neonatal intubation and uterotonics and packing and a kit for emergency bedside cesarean under local, like all of those things. But they didn’t specify, so it might. It could just have just a Doppler and a crash cart and a call button, of course, and that could be overseen by maybe a former LND nurse, not staffed by a single person that actually has OB experience, just probably some really good, well-rounded ER docs, but nobody that’s actually an OB and that would technically satisfy this CMS requirement, although we know that without the actual trained staff it still falls far below even the minimum level of basic maternal care that’s been set forth by ACOG and their obstetric care consensus.
Antonia: 25:58
So, going by this, women would be delivering in hospitals, potentially where nobody knows how to do a C-section or manage a postpartum hemorrhage or shoulder dystocia or cord prolapse, let alone an AFE or any number of other OBGYN emergencies that we’re trained to take care of in residency.
Antonia: 26:18
Like these are our bread and butter, and I know that nobody out there actually thinks that this is the goal that now these rural women, they can just maybe get a mobile unit to do their prenatal care and then they can go to the ER, to this little bed and deliver and everything will be great. That is obviously not the goal. But my hunch is that, as you said, budget neutral, like internally, they realized how tall of an order it would be to actually promise what is actually needed an actual OB unit with obstetricians, midwives and the whole thing. So instead they promised only what they thought was feasible right now with no money attached. So we have to ask whether that’s. Is that a constructive step in the right direction, there’s the right intention and right thoughts, or is it just a distraction and a pull away from what we do need to be working towards? And I suppose it could go either way, depending on how it actually gets implemented.
Howard: 27:12
Yeah, politics is a messy thing, but unfortunately, as part of we’ve got to address this stuff and we have to tackle it. So I mean, the things that put obstetric units at risk of being closed are the same things mostly that threaten the overall stability of hospitals, in rural hospitals in particular urban hospitals too in many cases, but rural hospitals in particular. I’ll put a link to a website run by the Center for Healthcare Quality and Payment Reform that goes over some of these issues. These are ultimately financial issues, although there are potentially lots of other things that come up, but most hospitals and most physicians do what they are financially incentivized to do. They say that about 30% of all rural hospitals are at risk of closing in the near future, which is about 700 of those hospitals that we had in that article, and that the approach of closing down service lines or certain inpatient services like obstetrics, or receiving one-time grants or shared savings programs with larger hospitals and things like that ultimately won’t prevent these closures.
Howard: 28:13
They’re just band-aids. This is what you see large hospital systems often doing, but they are just band-aids that kick the ball down the field a little bit but ultimately don’t prevent the closures and some of these one-time payments and things like that or some of these cutting service lines. What they do is they ultimately erode the stability of the hospital, and so the inevitable still happens Payers, particularly commercial insurance companies. They have to change the way they pay rural hospitals, and Medicare has to reverse its policy of paying more for services in urban areas than they do in rural areas. Medicaid programs have to pay a sustainable payment rate as well, since most hospitals and physicians lose money when they treat Medicaid patients, and Medicaid patients are disproportionately located in rural areas, particularly when you talk about obstetrics.
Antonia: 29:04
Yeah, that website, ruralhospitalschqprorg, identifies 19 hospitals at risk of closure in our state, Tennessee, but it’s a fairly bleak picture just across the country and we’re moving towards the legislative season now. I know you work on these issues through ACOG and our listeners really should also advocate for necessary reforms with their own local, state and federal elected representatives. This is a critical time right now. So, wherever you live, if you’re in the US, you’ve probably got some hospitals that are at risk nearby, and your politicians need to hear from especially doctors and patients that this is a priority that really needs to be addressed.
Howard: 29:52
Right and we need to reject these band-aid fixes. We need sustainable, vibrant, viable hospitals in our communities that aren’t constantly on the chopping block and at threat of closure.
Antonia: 30:03
Yeah, and we need money.
Antonia: 30:05
They need money and soon we can also talk about.
Antonia: 30:08
There’s other factors besides money here, but there’s a 2016 analysis published about why obstetric units, especially in rural areas, have closed, and it really is just one thing it’s a large medic Medicaid population that a lot of these hospitals have too few deliveries to break even and stay in the green. And, frankly, a lot of insurance payouts usually Medicaid and state, but then also a lot of commercial ones it’s just shameful. They don’t pay what it costs, they weigh underpay, and then when you primarily happen to have patients with those insurances that don’t cover the cost of basic essential care, then ultimately that hospital it’s just going to fail if they keep going down that road. And so then, of course, the obstetric units and every single patient who enters those units is going to be viewed by those hospitals as a threat to their survival and stability, because every time it’s costing them money. But that whole thing is just an artificial problem created by the payers and it’s a very short-sighted viewpoint that doesn’t account for long-term value and societal benefit of continuing to provide obstetric care.
Howard: 31:41
Prepare generalist OBGYNs for a real full scope of practice that you might see in a more rural setting, or even restrictive abortion laws if you’re in a particular state. These are definitely all serious issues, but they’re not the core problem and, yes, it is difficult to recruit a new OBGYN to a rural hospital.
Howard: 32:01
Ask me how I know, when that hospital itself appears to be at risk of closing, or when they see stories about women in that state dying from septic pregnancies because doctors are threatened with jail time if they provide lifesaving interventions 24-7, anesthesia or pediatric coverage OR availability or ultrasound availability 24-7,. Not even to mention the ability to manage miscarriages and ectopic pregnancies and other pregnancy complications that sometimes require abortion care. Well, yeah, they’re less likely to go to a place where those services are restricted or at risk of being lost. But bottom line is, most of the things that really keep doctors from choosing to go or incentivizing them to go somewhere are related to the stability of the hospital and the ability to pay those doctors what they should be paid in those settings. So we have to stabilize the hospitals, stabilize the payment system and then create the incentive structure for doctors to want to practice in these areas, and maybe more so in the light of those other headwinds.
Antonia: 33:08
Yeah, it’s a really scary thing for a brand new graduate to think about going somewhere where they just have no help, no good backup. It’s just on so many levels. But they’re going to be really worried about liability and about their patients maybe dying because they just don’t have the help that they’re used to in their training. And yeah, we haven’t really done a full, long dive on the abortion stuff lately for a while. But I think maybe some doctors will self-select to go to places in states that have really full abortion protections. And then there’s others that may conscientiously feel better about not terminating viable pregnancies and they’ll willingly go practice somewhere that’s more restrictive.
Antonia: 33:58
But everyone still needs to advocate for being allowed to terminate a pregnancy when the mother’s life is at risk, when she’s going to die. And there’s we know it’s not a black and white thing rape victims, that kind of thing. We need to be able to advocate for it and a lot of the cases that we’ve been seeing in the news horrible stories of moms just in the hospital dying because no one will touch them. There are stories relating to pre-viable PPROM where, instead of them thinking that they’re going to save the baby by not terminating it, they just lose both. They lose the mom and the baby. So that point is bigger than any one of us. It goes way above us and we just have to stay engaged with the politics of it, however we can and fight for our patients.
Antonia: 34:48
But best case, let’s say all abortions in the US to save a mother’s life, for example. Let’s say best case, that’s fully protected, no questions asked. Yes, we’re going to save her life, even if it requires an abortion. There’s still other issues with rural access to OB care. That would be a really great thing to happen in the US, but we would still have these maternity deserts. And so there’s things that can be done to help improve recruitment, like maybe extra student loan repayment efforts or bonuses or those kinds of incentives. But those are also like band-aids that don’t ultimately fix the problems that lead to not having ultrasound available after certain hours, having to be on Q2 call or Q3 call and constantly having a strained, understaffed unit constantly being at threat of closure. Nobody wants to live and work that way. So you see people leaving and relocating away, or maybe you see early retirements and then the whole unit shuts down because there’s just no doctors to staff it. But that original problem all comes down to the fault of our very perversely structured payment system.
Howard: 36:03
Yeah, there was an article in the New Yorker called the Texas OBGYN Exodus recently and it encapsulates all these things you’re talking about, and they did focus a lot about abortion in that article, but the main problem was they were taking care of a underserved community of patients who were either unfunded or had Medicaid funding, and the hospital just couldn’t figure out how to do it and they lost this whole academic program and this whole group of doctors over what, ultimately, is money.
Howard: 36:35
Yes, the other issues are a part of it, but those were things that you could work through and continue to build on if you could actually sustain this residency program. It was ultimately about money. So, yeah, there’s a lot of things to work on, but and we need to continue work on medical malpractice crisis and, yes, these restrictive abortion laws and things that don’t make sense for patient care and so many other things that just lead, in general, to physician burnout and create a bad environment for the obstetric workforce. And those issues, by the way, are things that affect both urban and rural hospitals and have a significant negative effect on our profession as a whole, and have a significant negative effect on our profession as a whole, but they’re not the root cause of why the rural hospitals in particular are losing access to obstetric care and why we’re seeing this crisis of maternity deserts in the US. This gets back, ultimately, to funding.
Antonia: 37:27
That 2016 article I mentioned. It has several quotes from respondents to their surveys about why their rural obstetric units closed. So I’ll just read them out and they really just completely illustrate these points. So one person says the one OB we had retired and moved out. Another one says our facility stopped doing OB, mainly based off of the inability to maintain consistent surgical and anesthesia coverage.
Antonia: 37:53
Another says we had two doctors anesthesia coverage. Another says we had two doctors. Then one stepped away and we had a hard time recruiting another one. We had trouble with coverage for anesthesia as well. It was based on low numbers and high malpractice insurance. We were purchased by another system and it was a financial decision to close the OB department. So I’m sure there was a insurance payout kind of issue there. The OB department closed due to budget cuts and also because there were other OB providers fairly close by. It wasn’t making any profit. We were in the middle of a financial turnaround and the new administration decided to stop OB care for financial reasons. And another one just says 80% of patients for Medicaid and 10% were no insurance, no pay.
Howard: 38:40
Yeah, and that study. They found that when a unit closed the average patient needed to travel about 30 extra miles for a prenatal visit or to get to a place where there was obstetric care, with some having to travel much further. 30 miles on country back roads is not 30 miles on the interstate. I mean in terms of time commitment, that might be close to an hour commute one way and if a woman has an average of, say, 13 prenatal visits, you’ve asked her to drive an additional 26 hours for what sometimes seems like a five-minute visit.
Antonia: 39:11
Yeah, that’s a lot of extra gas money and time off work and extra child care. That all comes completely out of the patient’s own pocket. That’s definitely not covered by insurance and there’s so many more things going that extra commute that can make her late or miss an appointment, like if there’s a tree down and now she has to reroute. Now she’s late. Now they have a late policy Show up 15 minutes late, you have to reschedule and then, in a true emergency, if she lives two hours away, she might not make it in time.
Howard: 39:42
Yeah, and ironically the folks who are the ones that live right next to the hospital are the ones who can stand to wait home a little bit longer, because if they do get out above their skis a little bit, they’re just a few minutes from the hospital. But these rural patients are the ones who can least afford to travel those distances but also least afford not to when there’s a problem.
Antonia: 40:01
Yeah, like they don’t want to come for a labor check if they’re not actually in labor and then drive all the way back, but yeah.
Howard: 40:07
So then they wait and have the baby in the car.
Antonia: 40:10
Yeah no-transcript.
Howard: 40:36
of course, certified nurse midwives who work in labor units or birthing centers and they’re part of the solution to overcrowded urban obstetric units for sure, but unfortunately I don’t think they’re a viable solution to low volume rural obstetric units. There needs to be a certain volume of deliveries to justify and pay for having both a midwife and an obstetrician on call. If you’re at a busy urban hospital with several deliveries a day and a doctor always on call, then midwives definitely help make that workload more manageable, and the doctors still have to be on call, though regardless, in order to do that emergency cesarean or operative delivery. That comes up something like that. But a rural hospital in a financial crisis that handles one delivery a day or less well, they can’t stay afloat financially if they hire both a doctor and a midwife to cover that three quarters of a delivery a day. So if the only other alternative is no obstetrician at all, you can see how many hospital CEOs would rather just shut the unit down.
Antonia: 41:34
Yeah, then hire both midwife and OB at all. You can see how many hospital CEOs would rather just shut the unit down. Yeah, then hire both midwife and OB. Yeah, and that’s what I was talking about. Is the certified nurse midwives. I know that term can also be used to refer to other types of people that use the term midwife, but they may be lay midwives or people with other type of training that are more focused on home births. They may not have any formal medical training at all. Midwives or people with other type of training that are more focused on home births, that they may not have any formal medical training at all. I was not talking about that as just to be clear.
Howard: 42:00
Yeah Well, and we don’t have to get in now into the issue of whether hospital or home delivery is safer for the purpose of answering addressing this question.
Howard: 42:09
Let’s just say, though, that you accept the argument that, for many low riskrisk patients, home birth midwives, certified professional midwives and others who are appropriately trained can provide an acceptable level of safety for those patients.
Howard: 42:22
That is better than delivering, say, with no care at all, or maybe in their car on the side of the road, that sort of thing, and that’s definitely a valid argument for someone who lives two hours away from the nearest OB unit. So, just for the sake of argument, let’s accept that premise. Well, you still need to understand that 16% of intended home births are transferred to the hospital during their labor process, and usually at a very late or emergent stage as problems have been developing. So we know, for example, that home birth in European countries is consistently safer than it is in the United States, primarily because of the proximity of the home to the hospital, and many have actual requirements about how far away you can be from the hospital and then the availability and sustainability of rapid and safe transport if something should go wrong. But if a home birth midwife is doing a delivery two hours from the nearest birthing center or hospital, or even an hour, then you will absolutely see an increase in neonatal and maternal mortality as that becomes more common.
Antonia: 43:22
Yeah, I agree with that. So what about midwife and doula led birthing centers? This is something that some public health advocates have been talking about as a solution in some maternity care deserts.
Howard: 43:35
Yes, and unless these birthing centers are within about 10 minutes from a fully equipped OB unit that’s capable of emergency cesarean and massive blood transfusion and neonatal resuscitation and intubation and umbilical lines and all those other things, then this is just as short-sighted as the CMS requirement that we talked about of requiring Doppler’s and the ED as a solution to the crisis. So I guess we have to ask the question of whether it’s better to have a midwife staff birthing center in a rural area compared to nothing. And yeah, okay, yeah, the answer is probably yes, right, because you can put some kid in there and train folks and standardized processes and things like that. But this idea also has the eroding effect on the stability of rural OB hospitals, because those birthing centers will attract away volume of patients, which diminishes the number of deliveries available to the hospital and makes them even more financially unstable. So in this model, all you’ve done is move the deliveries from someone’s home into a freestanding birthing center, which is easier on the midwives, by the way, because they have all the eggs in one basket. And yeah, okay, that’s likely a step up. But the birthing center also falls short of the most basic level of maternal care if it’s not closely linked with a hospital where obstetricians can treat obstetric emergencies. So ultimately, women’s and children’s lives are still put at risk. A lot of what we do in obstetrics just frankly doesn’t matter, for I don’t know 97%, 98% of our patients, something like that, and I freely admit that In fact, I love talking about how meaningless if you listen to this podcast a lot of what we do is. But for that 2% or 3% you’re going to be really glad we’re there. We make a huge difference, a life and death difference.
Howard: 45:15
The number of women who die in the United States right now, when we talk about maternal mortality, with something over 3 million births a year, is fewer than a thousand each year. And the number who die from direct intrapartum or obstetric events, we’re really just talking about a couple of hundred. But that’s because most women do deliver in a hospital, or close to one at least, where they can be taken if the worst should happen, and that hospital has a labor and delivery unit with the ability to give blood and to do cesareans and cesarean hysterectomies and other advanced life-saving interventions for the mother and the baby. This is true just as true for the newborn care that’s available there as it is for the mother’s care, and if we move deliveries out of the hospital setting into freestanding, unattached remote birthing centers, it might only increase the risk of maternal deaths by maybe one per thousand or so. But appreciate that’s an additional three to four thousand women a year dying in childbirth who don’t currently die.
Howard: 46:12
When you think about how many deliveries a year happen in the United States and for all the headlines that talk about our maternal mortality crisis, where the number of women who die in childbirth of a direct obstetric event is really just a couple of hundred, imagine if all of a sudden that number was in the three or four or five thousand range, and with that will come a similar increase in neonatal death and disability. So the folks who argue that essentially getting away from what’s called an obstetric model of care in the United States is the solution to any of this either are uninformed or simply are taking a macroeconomic, financial view of the problem where they don’t see the cost benefit of supporting the current obstetric model of care in the US. Cost benefit of supporting the current obstetric model of care in the US just to save a few thousand women and babies each year, because we spend money to save a few thousand women and babies a year and people need to pay for that.
Antonia: 47:03
Yeah, so maybe we should just have those birth centers in the hospital and so, in other words, just have L&D units in hospitals.
Howard: 47:10
That’s right, exactly yeah. Staffed with highly qualified and trained individuals, including midwives.
Antonia: 47:16
Yeah, trained midwives and doulas are definitely an essential part of our obstetric care delivery system and they should play an even bigger role than they currently do. And for a huge number, a huge majority of patients, they may honestly never even need to meet an OBGYN even once. And that’s exactly how it is in a lot of other developed countries too. Like well, someone out there can correct me if I’m wrong, but the UK or Finland, for example, midwives are the default and they’re the first line for prenatal and obstetric management, and then the obstetric physician gets involved for the operative cases and the complicated cases as a backup emergency. The OBGYN doctor and their operating room team and anesthesia services will be the difference in whether the mother or the child lives or dies.
Antonia: 48:20
And yeah, that’s not that many deliveries a year where we make that big of a difference, but when we do make the difference, it’s life or death. That’s how I’ve heard anesthesiologists jokingly say 95% of their job is just boring, and then 5% is like panic. I wouldn’t say panic, but you know, now it becomes life or death all of a sudden. So birth moved to being primarily in hospitals, because that’s where these lifesaving resources are and that’s where the trained people and teams are that use these resources correctly and maybe you can tell us more about that transition from home birth to hospital birth in the history?
Howard: 48:57
Yeah, I will, sure. I just want to wrap up, though. Let’s wrap this topic up first. I will say too, when people compare European birthing practices which hey, I’m all for the geography is always important to remember. You mentioned Finland. Well, Finland is barely bigger than the state of Arizona, and all of those women with midwife attended care are just minutes away from some of the most advanced obstetric and labor and delivery units in the world and qualified doctors to take care of them. So it is not a substitution, it is an augmentation. Now there’s a lot more we could talk about, but I want to clarify again that this is ultimately a problem of money. All the other issues start to get better when the money is distributed correctly.
Howard: 49:40
Right now, our US health care system does not prioritize the health of women and children. Pediatricians are among the lowest reimbursed of all physicians, and pregnant women and children are those most likely to be on Medicaid at a time when Medicaid pays cents on the dollar compared to commercial payers and even compared to Medicare. Those most likely to be on Medicaid at a time when Medicaid pays cents on the dollar compared to commercial payers and even compared to Medicare. Hospitals and doctors can make a profit on things like cardiology and cancer services and orthopedic services, which tend to favor older patients with commercial insurance, and of course, that is the demographic. That includes our currently elected officials and policy managers and all the folks who decide how and where our health care dollars are spent. We don’t have pregnant women and toddler moms making these decisions and running state and local government, because they’re busy actually raising the next generation of people. We have people who don’t care about women’s and children’s services making these decisions.
Antonia: 50:33
Yeah, just imagine if it was mainly, primarily, pregnant women in charge of the world. I think we should give this a chance.
Howard: 50:41
We’d have a different maternity system.
Antonia: 50:43
I guarantee you that.
Howard: 50:44
But, as you very well know, it’s hard to juggle child care that falls through at least half the time during flu and RSV season and then give your full attention to the kids when you’re at home. So our obstetricians know this. Moms like you who balance work and very busy at work and family time, we need child care. We have people who can’t work because of child care. We need this kind of representation in our government and in our policy institutions to make different decisions. But as it is now, women and children are basically an afterthought as far as health care resources are concerned, and that’s just true. They get relegated to this largely Medicaid-dominated system. That’s not sustainable and requires the hospital system or the physician practice to take a loss whenever they accept or treat one of those patients, and that’s just unacceptable.
Antonia: 51:30
Yeah, for deliveries, commercial insurers may pay more than three times as much as Medicaid does for the exact same service, and I just do not understand the logic of how can Medicaid say, yeah, we’re not really going to pay what this costs you, but you still have to do the service anyway. So apparently, I’ve been told it’s not just maternal care. The state insurances also don’t pay for a lot of other basic things too, like fixation of broken bones, for example, or at least in Tennessee. Someone out there can correct me, but I was surprised to hear about this. This was from an internal meeting with someone in our organization. But most pregnant women in the US do have Medicaid, and in the rural areas, as we said, that might be the majority like 80 or 90% of the patients have Medicaid. That is all underpaying for that service.
Antonia: 52:21
So then you create this system where many OB offices and hospitals will do everything they can to avoid Medicaid patients if at all possible, because they don’t want to go bankrupt.
Antonia: 52:31
So they can say, oh, we don’t accept that insurance, you have to go somewhere else. And ultimately some other doctors or hospitals will have to take one for the team, so to speak, because they feel that somebody has to deliver this baby right, and then they may be the ones that get saddled with all the Medicaid patients in that region and all of the losses that come with that, and that can create a different kind of care gap too, where, let’s say, it’s even in an urban area where a patient might live five miles away from an OB unit, but that’s the unit that doesn’t take her insurance, so she still has to go way too far away just to get care and again that’s access that’s blocked for no good reason. There’s just no good reason for poor reimbursement for pregnancy care. Things like this can absolutely get fixed when legislators prioritize women and children and move dollars in the healthcare system to adequately take care of them.
Howard: 53:30
Well, if we’ve gotten you riled up with this episode, then at the end here, take a minute to email your local, state and federal senators, representatives, congresspeople, right now and let them know that this is a crisis that you care about and want to see addressed and certainly, if you’re an OB-GYN, include stories of how your patients and your community are affected by this problem. It’s really time to act. It’s been time to act for a long time, but we’re now at a critical junction where these closures are accelerating and patients are suffering because of it.
Antonia: 54:00
Okay, well, we mentioned how most births went from being in homes historically to being in hospitals. Do we still have time for this quick historical tidbit?
Howard: 54:09
Yeah, let’s do it.
Antonia: 54:10
Okay, well, so there’s still some very vocal people out there maybe just the minority who really seem to romanticize this home birth scenario, and they like to talk about hospital births as being purely harmful, paternalistic, over-interventional kind of thing. So why don’t you fill in the story a little bit here?
Howard: 54:31
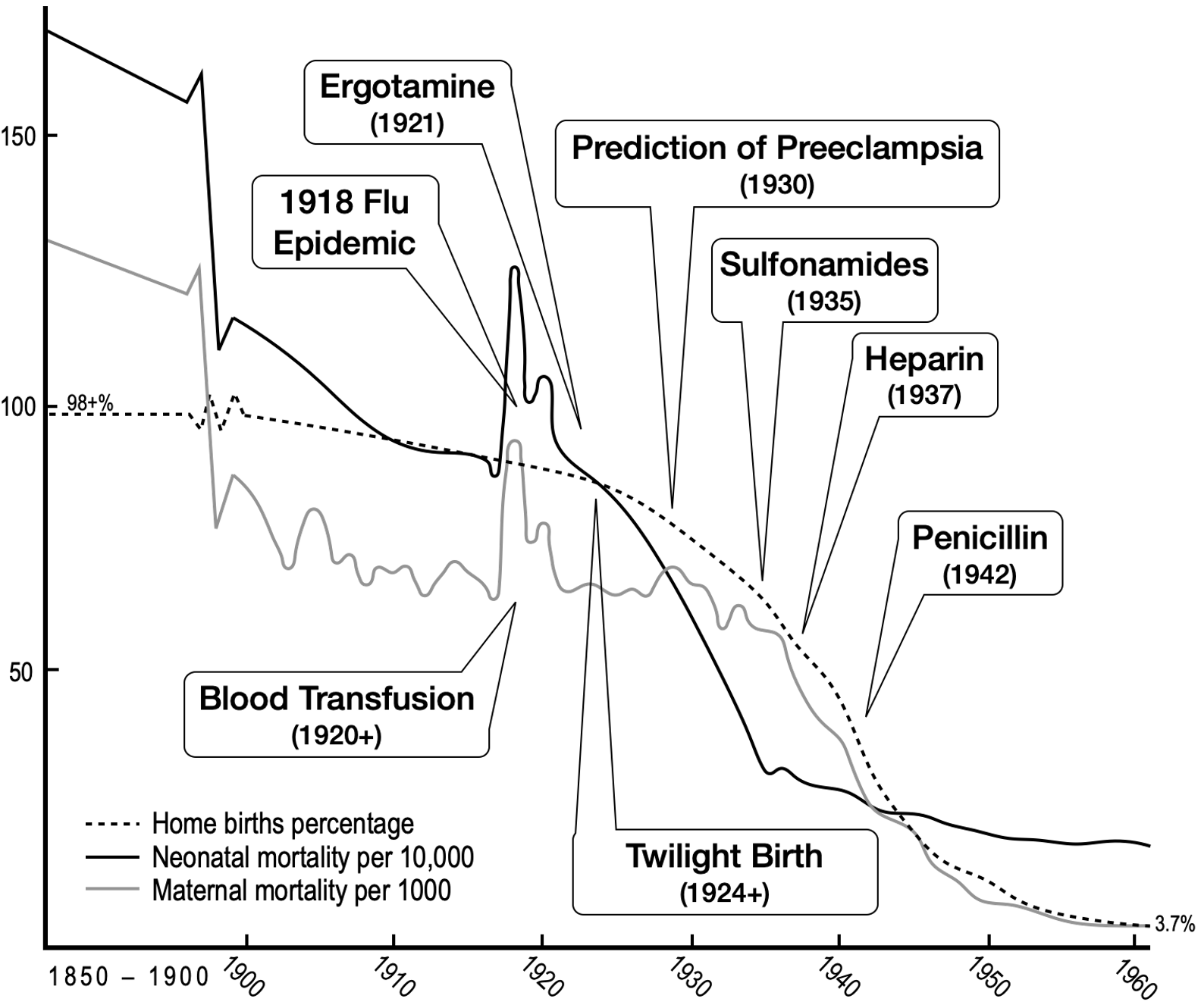
Yeah, and it’s complicated and the reasons for it, I think, changed over time and we don’t have too much time to spend on it, but I will have our Instagram. Ninja put a picture that shows the transition of home birth over time to the hospital, the rates of that and the concomitant decreases in maternal and neonatal mortality, along with some of the interventions that were leading to those improvements in care.
Antonia: 54:53
Is this a graph from your new upcoming book?
Howard: 54:56
It is, but don’t ask me when I’m going to be done writing it.
Antonia: 54:58
Well, yeah, you do work at two rural hospitals, so I’m guessing five years.
Howard: 55:05
Yeah, well, we’ll see, but I’m definitely aiming for sooner than that.
Howard: 55:08
But essentially, if you look at the graph before 1900, something like 98% of births in the United States were in the home setting and many were attended by midwives. But increasingly many were also attended by just general practice, the local country doctor, if you will, who would go to the home when there was a birth. And at the time hospitals didn’t have much advantages to offer patients except maybe quicker access to the doctor or midwife. Just to offer patients, except maybe quicker access to the doctor or midwife. It was more convenient for them to have all the patients in one place, just like a birthing center is more convenient for the midwife today compared to having to go and sit in someone’s home for hours. Well, the same thing was just a pragmatic thing.
Howard: 55:46
So you largely saw in urban areas only poor women going to hospitals, particularly in the biggest cities where these hospitals started You’d have women who lived in tenements and small overcrowded homes or apartments where there just wasn’t even space to have a home birth, if you wanted to.
Howard: 56:01
So hospital births in that sense started out as a way of taking care of the poorest of patients who were all aggregated in one place. But then in the 1920s there were more interventions in hospital settings that just weren’t available to patients who were at home. This included anesthesia, which was becoming very popular then, and pain relief of some sort, which was enough, frankly, to convince large groups of women to go to the hospital because they wanted pain relief, but also things like ergotamines, which came out in 1921, which was an amazing, life-saving intervention to help treat postpartum hemorrhage. The other thing that we learned a lot about at that time was blood pressure. Like we discussed before, by 1930, we understood how to detect preeclampsia, and we understood that when you found this, they needed to be delivered. So it became a priority to check blood pressures and on women throughout their pregnancy to identify them and then, of course, maybe to deliver them, and then, of course, maybe to deliver them, and that would have been in a hospital setting.
Antonia: 56:57
Yeah, that’s still one of the most valuable things we do for pregnant women now and that’s really the basis of our modern prenatal care visit schedule is screen for preeclampsia.
Howard: 57:08
Right and it made a huge difference and patients saw the value of hospital birth because they all at that age they knew people in their family stories and in local communities who had bad outcomes from preeclampsia or other complications of pregnancy. So women embraced the idea of a prenatal care program that was designed to screen and treat and prevent women from getting eclampsia. But the 1930s, 1940s, in general, that was the miracle age of medicine. So sulfa drugs became available in 1935, and now women didn’t have to die of pure peril infections. And heparin became available in 37 to treat people with blood clots, and then penicillin in 1942, and so on. And all these things were at the hospital, along with that, anesthesia to provide safe operative deliveries for babies that wouldn’t come out spontaneously. Even cesarean delivery by, say, 1950, had become a very safe thing to do, whereas just 50 or 60 years before that nearly everybody that had one died.
Antonia: 58:06
Yeah, I’m looking at that graph that you mentioned. That’s going in your book, and maternal and neonatal mortality both dropped by like 99% in that 100-year span from 1850 to 1950. And so there were women up to the 1950s with these vivid, I’m sure traumatic memories of how bad it had been to have a baby at home, who embraced the idea of going to a hospital and not dying or not losing their babies during childbirth.
Howard: 58:37
Yeah, they did, and we don’t have that memory collectively in our conscious anymore. Same thing happens with vaccines you and I don’t know anybody who had polio, for example, so the value of it seems less. But they did. They went to the hospital and by 1960, only about 3.7% of women still had home births. In fact, the narrative flipped where at that time it was poor women who had out-of-hospital births, because anyone who could afford it wanted to be at the hospital. The same thing happened with breastfeeding too, where the narrative flipped from it’s interesting stuff, but they wanted to be at the hospital if they could afford to go and they were paying for it where the life-saving equipment and the well-trained nurses and doctors were located.
Howard: 59:16
And the modern midwife resurgence started in the US at about that time, actually to address the most underserved areas where hospitals weren’t available.
Howard: 59:26
And specifically it started in Appalachia, where the poorest and most underserved women in the US were located and midwives literally would drive army jeeps that they got brought back from World War II up into the mountains to provide prenatal care and obstetric services to women who didn’t have access to hospitals.
Howard: 59:43
That was not because they believed that they were providing a better service than the hospital could provide, but because these women just couldn’t get to a hospital if they wanted to and midwifery was the best option available to them in those rural poor areas. And this gap was perceived as a huge problem from a public health perspective, and Americans were increasingly upset that poor women and children didn’t have access to health care that other women and children did have access to. So in 1984, the Medicaid program was used to start paying for pregnant women to receive care and was expanded to cover more and more pregnant women by expanding the definition over time of who all would qualify for Medicaid. This allowed rural hospitals to open obstetric units in places where they never would have opened one before, to provide access to these pregnant patients and their children.
Antonia: 1:00:33
Well, that’s a bit ironic. That was meant to help pregnant women. So what happened to get us to the point where now they’re no longer paying for it, and now they’re the reason these units are closing?
Howard: 1:00:45
Yeah Well, I’ll put a link to a paper that looks at the economic policies here. That just shows what happened to Medicaid. But the really short version of that is the budget for Medicaid was never increased sufficiently to cover all the things that it’s been asked to cover as you add more and more patients to the rolls. So reimbursement has dropped year over year for obstetrics and pediatric services. Even if it wasn’t diminished, it didn’t keep up with inflation In the last several years, just acutely. Inflation has made this crisis much worse. We’ve seen just that. Everybody knows how much inflation has been over the last five years. It’s more expensive than ever to deliver care due to that inflation and the reimbursement from Medicaid has not adjusted at all for that, not in many years. In fact, it’s lower per delivery in adjusted inflation dollars than it has ever been in terms of covering obstetric and pediatric services.
Antonia: 1:01:39
Just got to adjust for inflation then. So okay. So all of that started with public outrage and pressure to get access for rural pregnant women, pregnant women. So I wonder if that’s what is needed again to pressure the system to fund, you know, pull money from somewhere else to keep these units afloat and to pay a fair price to all of the teams, the OBs and nurses and everyone and increase the budget so that pregnant women don’t have to go back to having these army jeeps trying to bring a little mobile home birth unit to them in a little duffel bag or something. We’re in the 21st century now and these safe interventions are available and they’ve been available. They need to stay available. So we just have to try not to screw that up, I guess.
Howard: 1:02:28
Yeah Well, press, stop on here and open up your email account and send off some emails and then keep doing it periodically to your local politicians and your state and federal representatives, so otherwise we’ll be back on Christmas with something. We’ll have to throw something Christmasy in.
Antonia: 1:02:46
Yeah, we’ll see you then. Something festive.
Announcer: 1:02:52
Thanks for listening. Find us online at thinkingaboutobgyn.com. Be sure to subscribe. Look for new episodes every two weeks.
